
Prather H. What puts the “morbid” in morbidity: A call to reform the way we address weight in the exam room. HPHR. 2021;53.10.54111/0001/AAA5
In 2003, U.S. Preventative Services Task Force (USPSTF) made the first official recommendation that clinicians ought to “screen all adult patients for obesity and offer intensive counseling and behavioral interventions to promote sustained weight loss for obese adults.”13 Since then, number of patients who meet the clinical definition of overweight or obese has continued to increase. Indeed, the most recent statistics show that 80% of adults and 1/3 of children are now classified as overweight or obese and weight counseling is therefore likely to be experienced by most patients in the exam room. This essay is a commentary on medicine’s history with bias against overweight individuals and why the current approach to weight management is harmful instead of helpful, supported with anecdotes from my own experiences. Indeed, as a medical student whose experienced overweight-bias as both a patient and a medical trainee, and I am calling for reform in the way we have conversations about weight in the exam room because it represents an opportunity to avoid morbid consequences for a population that is being actively harmed by biased communication skills.
Venus of Willendorf
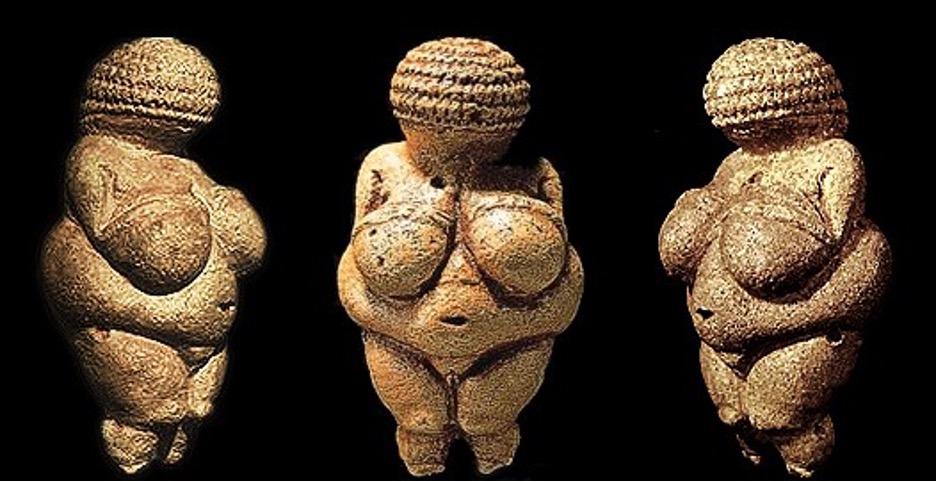
I can vividly recall sitting in an art history class in college and learning about “The Venus of Willendorf.” It is a prehistoric statuette from the Paleolithic era of a small feminine figure with a large belly, ample hips, and pronounced breasts (Figure 1). It’s thought that she existed as a fertility statue and that women worshipped her figure and prayed to her as a deity. But what stands out to me most about her is how similar her body looks to so many bodies I’ve encountered during my medical training and how drastically the social response to bodies like hers has shifted over the last 30,000 years.
The modern-day attitude of medicine is that obesity is an out-of-control evil that needs to be defeated from inside the exam room. Again and again, I see use of generalized one-liners like “being this heavy is bad for you”, “what are we going to do about that weight”, or “you need to lose weight”, as if each of those unsolicited statements haven’t run through the minds of all overweight patients many times before. These conversations and labels are then qualified behind closed doors by saying it’s a medical fact as if facts do not hold the power to be harmful. We rely on objective measures to talk about weight – namely BMI – but weight is a subjective, dynamic, and multifactorial experience. When you see an overweight patient sitting in front of you, you cannot know just by looking at them how they got to this spot in life. Other health conditions, hormones, the microbiome1, genetics, trauma, disability, depression, and various social determinants of health can all be at play simultaneously, and a quick one-liner during the last few minutes of an encounter to document “weight counseling was given” cannot possibly be enough to identify the barriers to weight loss. As a medical student whose had the privilege of experiencing this bias as both a patient and a medical trainee, and I am calling for a change in the way we have conversations about weight in the exam room because it is actively harming patients.
I went on my first diet when I was 10 years old. My mother started me on Weight Watchers early in life, hoping to save her overweight daughter from the social difficulties that come with being in overweight woman. Each day I counted my calories, writing wheat toast and sugar-free popsicle in my food diary and wishing my body looked different, while other kids ate Lunchables and Oreos shamelessly. I lost 20lbs for the first time before even starting middle school, and this was just the beginning of a complicated, ongoing journey with my body image and beauty standards.
As an entity, medicine is not responsible for society’s obsession with beauty standards or the pitfalls in the way unhealthy body images are pushed on children, but it is complicit in perpetuating those effects by having biased or unwanted discussions about weight with its patients, refusing to acknowledge biases against this population of patients, and justifying it by using “healthiness” as a disguise. In fact, medicine has a long history with bias and prejudice against overweight individuals2. For example, the CHANGES study2 conducted in 2014 showed that 67% of medical students exhibit weight bias. This figure is particularly disturbing to me. Consider how today’s medical students are tomorrow’s physicians and question, what are we actively doing to combat these biases? We use metrics like the Implicit Association Test (IAT) to prove they exist, but how are we preventing it from following us into every clinical encounter. Moreover, we know that these prejudices come out of the woodwork all the time, with many physicians believing that “teasing or criticism will motivate such patients to lose weight, unaware that negative experiences compel people to eat more and further increase their weight, establishing a vicious cycle.”3
By 16 years old, I was eating 900 calories a day. My snack of choice was ice, dessert was sugar-free gum, and I was eating one meal a day. Was I an emotionally labile teenager? Sure. But I was also desperately trying to fit a strict social standard, and deep down I knew I would never be a girl who was “effortlessly thin”. I quickly dropped 40lbs and was proud to make an appointment with my doctor, eager to show her how well I had done. She didn’t ask me if I was exercising. She didn’t ask me what I was eating. She gave me a quick, “keep up the good work, let’s do another 40”, before concluding our encounter.
To some degree, I can’t blame my doctor for keeping it brief. My BMI was still in red on the side of the chart, and a quick comment was really all that time allows when there are multiple items on the agenda. The average outpatient encounter is slotted for 15-20 minutes, which should be the amount of time spent on weight counseling alone. To get a clearer picture of a patient’s habits and barriers takes time, and 15 minutes simply isn’t enough. More to the point, these brief and incomplete conversations regarding weight aren’t just imperfect, they’re actively causing harm to overweight patients, particularly women. And if we are not going to do them well, or if they are unwanted by our patients, then we should save them for those with the time for a trauma-informed and bias-free approach.
These conversations are doing more than just stigmatizing our overweight patients. It’s been shown that “patient–physician communication influences patient behavior”4, and when communication is poor, it keeps patients from adopting healthy behaviors. Not only do physicians who have less respect for particular patients build less rapport5 and express a less positive affect6, but another study showed that half of overweight women, “had cancelled or delayed a doctor’s appointment until they could lose weight”7 because they dreaded having to confront their doctor about it.8 Another showed “patients with diabetes who reported lower trust in their physician were significantly more likely to be non-adherent to their hypoglycemic medications.”9 Frequently, these patient behaviors are attributed to stigmas and biases about laziness and willpower, but more importantly they are a direct extension of poor communication and weak doctor-patient relationships. Furthermore, it tells me that many patients simply don’t want their weight brought up. One Huffington Post article put it perfectly, “doctors are supposed to be trusted authorities, a patient’s primary gateway to healing. But for fat people, they are a source of unique and persistent trauma”.10
Our cultural obsession with appearance is leading doctors to disproportionately focus on weight and to interact with overweight patients differently from thin ones5,6. And with 80% of adults and 1/3 of children now being classified as overweight or obese, this means the harm isn’t just being encountered by many, its being encountered by most. Consider the story of Rebecca Hiles. A young girl who developed shortness of breath in the setting of obesity. She was diagnosed with many things: asthma, GERD, and most importantly, her weight was consistently brought up at every encounter. She saw several doctors and yet her symptoms continued to worsen. She was eventually diagnosed with a cancerous lung tumor that several doctors had missed, despite her insistence that there was something more serious going on. This story serves as a lesson for doctors are missing important diagnoses because of their focus on a patient’s weight as an explanation for any chief concern.7 This was not a one-off event either, secondary screenings are frequently delayed in obese women10, and they are more likely to die from breast cancer and cervical cancer because of this.11 One story that is particularly disturbing to me is that of an OBGYN clinic in south Florida that was turning women away if they are over 200 lbs12 which, to reiterate, is going to be a significant portion of women.
It is not that we should never have these conversations. In fact, as someone in favor of holistic approaches to health, it would be hypocritical to say we should ignore weight despite its effects on health. I also recognize that my experiences may not be representative of the efforts of all physicians, and there may be many out there conducting these conversations appropriately. Whether this is the case or not, the truth of my experiences leads me to believe that the execution of weight counseling in practice is generally poor, and its overall impact on the populations we claim to care about is causing harm to our patients and eroding the trust that underscores doctor-patient relationships. As opposed to stimulating pre-contemplation and a healthy lifestyle, it pushes patients further from health, further from wellness, and further from their providers, thus robbing them the opportunity to have otherwise gotten adequate care and further stigmatizing them. I’ve seen some discussions that emphasize the stance “this isn’t just about hurt feelings” but has morbid consequences. But I maintain, why can’t it be about both? Overweight patients deserve to feel safe and cared about when sitting in front of their doctor, and every encounter should be free from discrimination and provide equal care for all patients. In this era of queer rights and acknowledgement of systemic racism in healthcare, there is ample discussion about how to make certain marginalized populations that have historically been wronged by medicine feel safe. I often see doctors wearing pins or buttons that say You’re safe here or with depictions of a pride flag or a black fist. But does this attitude apply to our overweight patients too?
It wasn’t supposed to be like this. While it’s true that the rules and regulations established by the U.S. Preventative Services Task Force (USPSTF) say that clinicians ought to “screen all adult patients for obesity and offer intensive counseling and behavioral interventions to promote sustained weight loss for obese adults,”13 but the evaluation of the efficacy of these conversations never incorporates mental impact or effects on doctor-patient relationships. Furthermore, these conversations were supposed to rely on the framework referred to as The 5-As: Assess, Advise, Agree, Assist, and Arrange14. This framework relies on open discussion with patients about their weight goals, their social barriers to weight loss, and providing them tools and information needed to change it. Paradigms like “Health at Every Size” are doing exactly this and are contributing to a movement working to promote size-acceptance, to end weight discrimination, and to lessen the cultural obsession with weight loss and thinness15. Being thin is not a requirement for respect, and doctors need to take action to change the way we conduct conversations about weight in the exam room.
Some concrete solutions I’d like to see is to put the power to set the agenda back into the hands of the patient. A step towards addressing the animosity and judgement felt by overweight patients in the exam room could be with the addition of pre-encounter questions to their review of systems paperwork they already routinely fill out. We should probe for interest on the topic of weight management and get a comprehensive picture of their diet and exercise barriers before the encounter and give back the power to decide if it’s talked about or not. Questions like: Are you satisfied with your current diet and exercise? Are you happy with your current weight? What are the barriers in place that are affecting you from changing your diet and exercise? Would you like your weight to be brought up in today’s appointment? This creates a more comprehensive picture of a patient’s wellness and lifestyle beyond an objective metric and is more in line with the “holistic view of health” medicine is shifting towards. We need to do a better job discussing obesity and put a greater emphasis on its multifactorial origins. I’ve rarely heard doctors talk about how obesity isn’t a choice when you consider all the factors I’ve outlined or that efforts to change one’s weight go far beyond willpower and lifestyle modifications. If a patient does indicate wanting weight counseling, I’d like to see “The 5-As” framework put into practice, with solutions to barriers follow-up plans that are tailored to a patient’s individual and unique needs. Furthermore, if a patient does not want to discuss it, a doctor will save that time in an encounter and can focus on other aspects of care instead. A patient gets adequate healthcare free from guilt and shame, a doctor has a better chance of staying on schedule, and the doctor-patient relationship remains strong.
Haleigh Prather is a third-year medical student and AHEC scholar at Oregon Health & Science University (OHSU) in Portland, OR. As a Latina woman who grew up in a low-income, single-parent household, her motivation for pursuing medicine stems from an interest in studying (and a history of living through) many of the social determinants of health as well as a curiosity in exploring medicine’s relationship with representation and identity. Specialty wise she is planning to go into pediatrics.
She grew up just outside Los Angeles, California and completed her undergraduate education at Vassar College in upstate New York. She then spent the next two years in Baltimore, MD to pursue a Master’s in Health Science in Biochemistry and Molecular Biology from the John Hopkins: Bloomberg school of public health.
She is a passionate advocate for equity and social justice, with an emphasis on having a more heterogenous population of students admitted to medical school. In addition to her studies, she is a part of OHSU’s student council, she is a senior leader with the Women’s Leadership Development Program (WLDP), and is a mentor with the Latino Medical Student’s Association (LMSA). She is also currently working on a scholarly project that focuses on development of an educational intervention to decrease rates of pre-operative anxiety among Spanish-speaking children to improve post-operative outcomes.
Outside of work, she enjoys building intricate Lego sets, watching marvel movies, crocheting and playing with her kitten Bongo.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.