
This trio of posts was inspired by the Health Effects Institute conference sessions on April 6th and April 20th, 2021.
***
There are many ways that climate change is expected to impact human health. Air quality is an important piece of this puzzle due to the links between climate change and air pollution, air pollution and health, and emissions of greenhouse gases (GHGs) with emissions of criteria air pollutants.
How might climate change lead to more air pollution affecting health? First, warmer temperatures in many parts of the world are expected to produce more ground-level ozone and certain kinds of particulate matter; the latter is due to increased wildfires and/or airborne dust, given drier land conditions. Second, some research has suggested that there will be more atmospheric stagnation events with the potential to trap air pollution down closer to where we breathe. Third, warmer and/or more humid climates are likely to increase people’s air conditioning use, triggering more electricity demand and power plant emissions (when fossil fuels are being used to generate electricity).
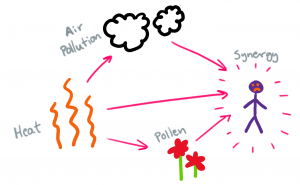
In addition to increasing air pollution, climate change might also worsen the health impacts of air pollution due to increased heat and pollen. Under climate change scenarios, both average and extreme temperatures are expected to rise. Also, issues with pollen may be exacerbated by increased and more rapid plant growth, increased pollen production by plants, increased allergenic proteins contained in pollen, longer plant seasons, and the aforementioned atmospheric stagnation events. These changes are especially concerning in combination with one another. A 2020 review found substantial evidence of a synergistic (adverse) health effect between air pollution and heat, and some evidence for synergistic effects between (i) air pollution, pollen, and heat and (ii) air pollution and pollen. Scientists are actively exploring other potential interactions between environmental and social factors exacerbated by climate change.
At this point, you’ve probably heard a lot about GHGs, and some about criteria air pollutants (described in my first blog). But how are reductions of these different emissions from human activities related? While traditional air pollution controls (such as those mandated by the US Clean Air Act for power plants and vehicles) have been quite effective in reducing criteria air pollutants, they have not regulated GHGs such as carbon dioxide (CO2), which is the primary driver of climate change. In fact, there are no analogous “end-of-pipe” technologies for limiting CO2, and many traditional air pollution controls can actually end up increasing CO2 emissions by lowering the efficiency of power plants through a heat rate penalty. By contrast, reducing CO2 emissions simultaneously limits emissions of criteria air pollutants. I’ll go into more detail on this in my next blog, exploring decarbonization strategies from the air quality + health perspective.
To what extent does burning fossil fuels contribute to ambient air pollution and the global health burden? A study published in June found that 1.05 million deaths in 2017 (95% confidence interval = 0.74–1.36 million deaths) were attributable to fossil fuel combustion, which generates 27.3% of the world’s PM2.5 burden (coal = 14.1%, liquid oil and natural gas = 13.2%). The figure below (from the same paper) shows the global distribution of deaths from ambient PM2.5, the fractions of PM2.5 emissions attributable to different sectors and fuel types, and the fractions of deaths from different diseases associated with long-term ambient PM2.5 exposure.
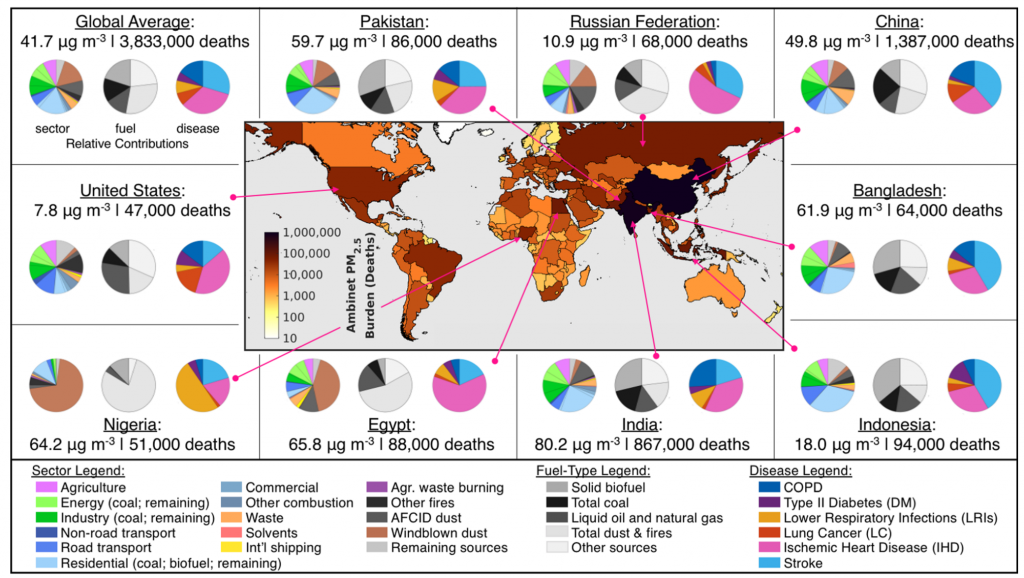
McDuffie et al., 2021, Figure 2: Absolute ambient PM2.5 burden and fractional sector, fuel, and disease contributions for the global average and top nine countries [those with the largest number of attributable deaths associated with long-term ambient PM2.5].
This study also found that although global emissions from coal have been decreasing in recent years, coal still contributes the most (compared to other combustible fuels) to the PM2.5 disease burden in 20 countries. Solid biofuels, used primarily for residential heating and cooking, contribute the most to PM2.5 disease burden in 78 countries. In addition to the estimated 1.05 million deaths from fossil fuels, 0.77 million deaths (95% CI = 0.54–0.99 million deaths) in 2017 were attributable to solid biofuel combustion.
In general, the authors observed that countries with the greatest PM2.5 disease burden had the largest relative contributions to air pollution from anthropogenic sources. For example, China and India, which between them are home to 35% of the world’s people, experience about 60% of the total global deaths attributable to ambient PM2.5, and their emissions from fuel combustion contribute to about 30% of this burden.
These results contribute to mounting scientific evidence of the potential “co-benefits” for health if fossil fuel emissions were reduced or even eliminated, meanwhile hinting at challenges associated with regulating air emissions, which I will discuss more in the third part of this trio of blogs.
***
Recommended: Explore source specific emissions and attributable mortality data visualizations accompanying the paper by McDuffie et al. (2021)
More on Ellen Considine here.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.