The menopause is a natural part of the female life cycle. But why do women become invisible after the menopause? Dr Jen Gunter answers my question 'Ain't I A Woman?"



The menopause is a natural part of the female life cycle. But why do women become invisible after the menopause? Dr Jen Gunter answers my question 'Ain't I A Woman?"
The menopause is a natural part of the female life cycle. But why do women become invisible after the menopause? Dr Naghat ARif answers my question " Ain't I A Woman?"

In this game of gonads, who decided that a testicle is worth more than an ovary?

To deputise a complete stranger to interfere with a woman’s health choice is constitutionally, medically, morally and ethically wrong. That's the end of my sentence.

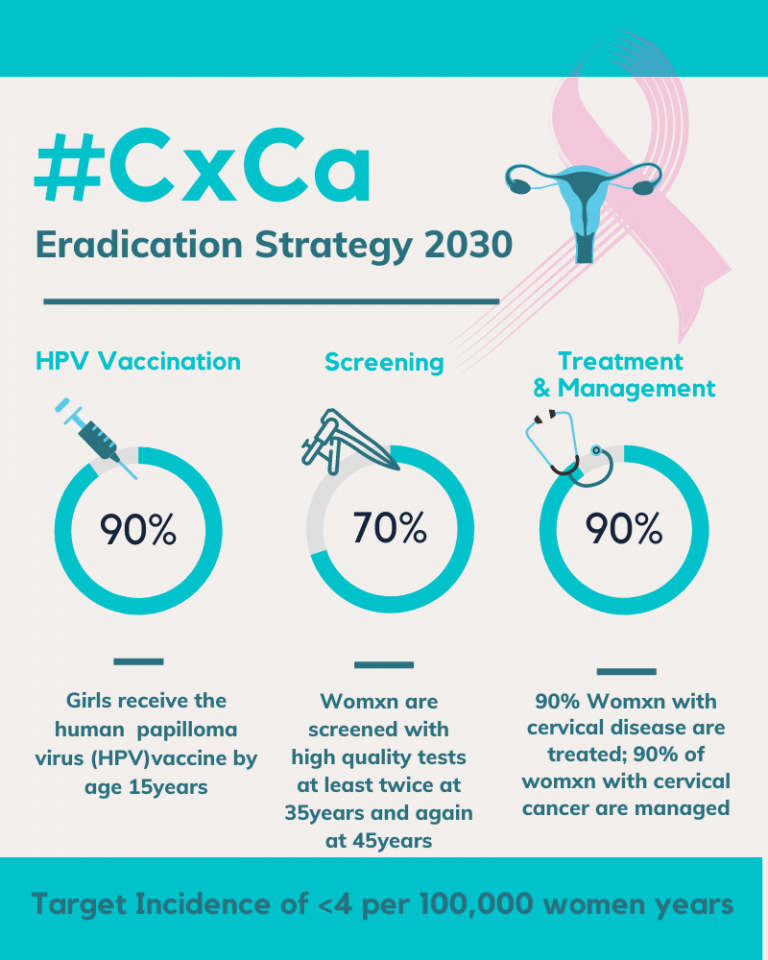
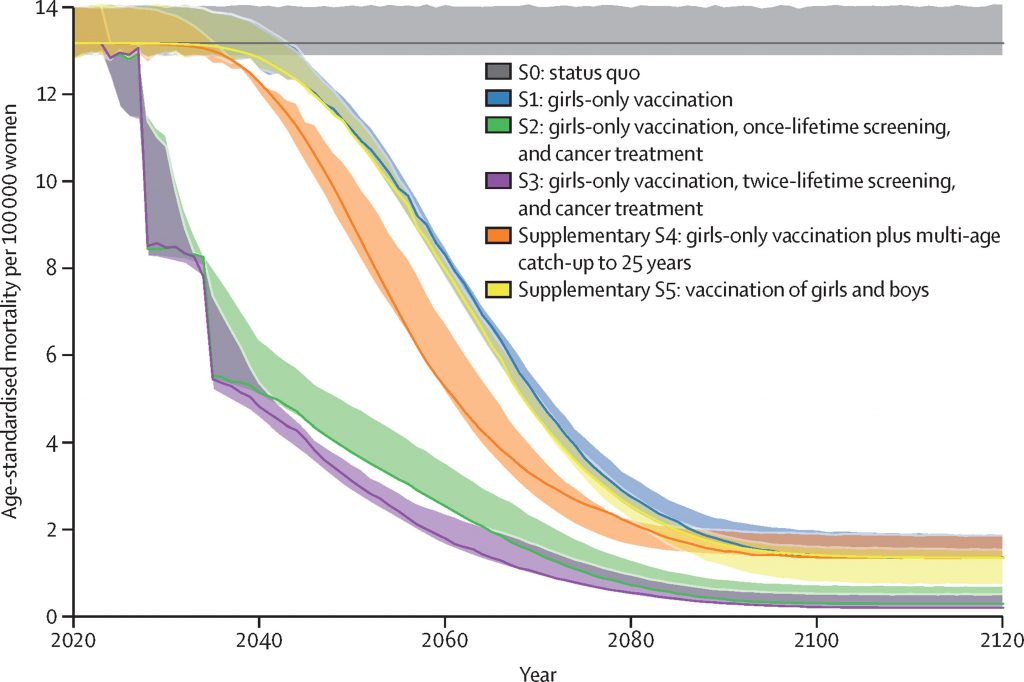
Cervical cancer can be prevented. When detected early it can be treated and cured with surgery. As we mark the one year anniversary of the "Cervical Cancer Elimination Day of Action", I reflect on the role of surgical systems in eliminating cervical cancer.

Adolescents make up 16% of the population and straddle the sometimes uncomfortable gap between childhood and adulthood. Seeking out information on the internet makes sense but at what cost?

Periods don't have to cost us education, equity and the environment

We had no say in the decision of when, how, where and to whom we were born. Yet this was one of the most important decisions in our lives, which continues to impact us today.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()