
Jimeno K. COVID-19 and the code: revisiting the Philippine experience. HPHR. 2021; 30.
DOI:10.54111/0001/DD24
The World Health Organization (WHO, 2020) recommended that breastfeeding of infants should be initiated and continued even among mothers with suspected or confirmed COVID-19. Lubbe et al. (2020) corroborated that the coronavirus is not transmitted via breastmilk and the benefits of breastfeeding disproportionately outweigh the risks during the coronavirus pandemic. Nonetheless, the formula milk industry has found a way to exploit panic and fears of contagion to increase sales by donating milk powder and other food, in violation of the WHO International Code of Marketing of Breast-milk Substitutes (the Code) and national law in many countries (van Tulleken et al., 2020). In line with the Global Breastfeeding Collective’s (2020) call to action, this article highlights why adopting the Code is a global health imperative and what contributes to its successful legislation in the Philippines.
The BMJ, a prominent medical journal, announced that it will stop carrying advertisements for formula milk (Godlee et al., 2019). The decision came after an investigation that exposed how the formula milk manufacturers had conspired with the authors of the guidelines on cow’s milk protein allergy (van Tulleken, 2018). The journal editors acknowledged that they were “reminded of the substantial harms caused by aggressive promotion of breast milk substitutes and the biases introduced into research and clinical practice by industry influence” (Godlee, 2019). The BMJ’s move is a strong statement against the shenanigans of the milk industry to advance its interests to the detriment of the public.
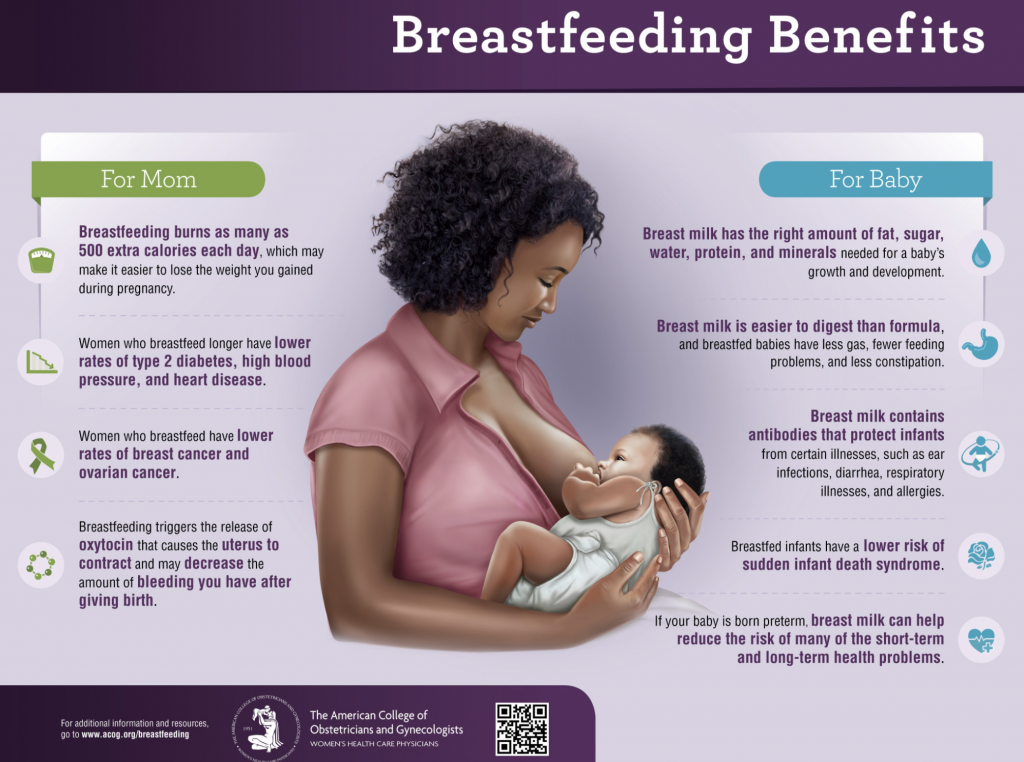
The literature is unequivocal on the benefits of breast milk to the mother and the baby. The American College of Obstetricians and Gynecologists summarized the benefits in the infographic below (see Figure 1). Exclusive breastfeeding for the first 6 months, without any formula milk, is therefore recommended by doctors unless the conditions justify that breastfeeding should be discontinued temporarily or permanently. Examples of these conditions include mothers with HIV infection and infants born with lactose intolerance, where a special galactose-free formula is needed. However, unethical marketing practices of the milk industry have undermined these findings and altered the public perception of breast milk contributing to the decline of breastfeeding rates around the world.
The Code was adopted by the World Health Assembly (WHA) in 1981 “to contribute to the provision of safe and adequate nutrition for infants, by the protection and promotion of breastfeeding, and by ensuring the proper use of breast-milk substitutes, when these are necessary, based on adequate information and through appropriate marketing and distribution” (WHO, 1981). According to the Code, a breast-milk substitute means any food being marketed or otherwise presented as a partial or total replacement for breast milk, whether or not suitable for that purpose. In effect, it bans the promotion to the general public of all milk products that may replace breast milk in the first three years of life. Formula feeding, on the other hand, refers to the infant consumption of breast milk substitutes.
Ratifying the Code is an economically sound policy because formula milk is more expensive compared to breast milk—a natural, free, and species-specific source of infant nutrition and health. Moreover, formula feeding has been associated with suboptimal breastfeeding practices among lactating mothers, resulting in an increased incidence of malnutrition and diarrhea among infants (Victora et al., 2016). A 2005 estimate by the United Nations Children’s Fund (UNICEF Philippines, n.d.) underscored the costs of formula feeding for the families and the Philippine economy. Formula feeding is valued at an average of USD 100 a month per infant and Filipinos spend almost USD 1 billion a year with prices adjusted for inflation. It also requires sterile water and shall be administered immediately to prevent contamination. To save on expenses, some families dilute the formula or use other kinds of milk (including condensed milk) leading to malnutrition, illnesses, and death.
There are hidden costs which include physician’s consultation, medicines, and hospitalization, often unaccounted to the burden of formula feeding. The costs of outpatient treatment for acute respiratory infections caused by formula feeding amount to USD 1.37 million per year, while hospitalization is worth USD 640 thousand annually (UNICEF Philippines, n.d.). The parents also have to miss working days resulting in loss of income. The total lost wages due to tending formula-fed children for diarrhea and acute respiratory infections during the first six months of life is USD 20 million. Funeral costs associated with child deaths due to formula-feeding and other inappropriate infant feeding habits sum up to USD 13 million.
Formula feeding is also detrimental to the environment because of the huge amounts of waste it generates: cans, cartons, feeding bottles, and teats. The limited milk production in the Philippines necessitates importation to meet the demand for breast milk substitutes. The country’s National Dairy Authority reported that the amount of imported milk rose to a record-high of USD 1.13 billion in 2019 (Arcalas, 2020). These indirect costs suggest that the Code is a value-for-money intervention every nation can adopt.
As of 2018, only 35 out of 194 countries fully implement the Code after almost 40 years since the WHA adoption (WHO, 2018). In Southeast Asia, only the Philippines and Thailand have full Code provisions covered in law (see Table 1). The Philippines is among the first countries that took immediate action after the WHA Resolution 34.22 by transforming the Code into national law. It is important to note that the Code was adopted as a recommendation rather than regulation, hence, it did not readily “come into force” for member states. The crux is that the Philippine version of the Code is not dependent on the age of the child but the kind of product being marketed to the public.
Table 1. The Code’s legal status in Southeast Asia
Country | Year of most recent legal measure | Legal status of the Code |
Brunei | N/A | No legal measures |
Cambodia | 2005 | Many provisions in the law |
Indonesia | 2012 | Many provisions in the law |
Laos | 2007 | Few provisions in the law |
Malaysia | N/A | No legal measures |
Myanmar | 2014 | Many provisions in the law |
Philippines | 2006 | Full provisions in the law |
Singapore | N/A | No legal measures |
Thailand | 2017 | Many provisions in the law |
Vietnam | 2014 | Full provisions in the law |
Philippine success can be traced to the confluence of events before and after the Code. During the early 1980s, second-wave feminism was gaining traction as women organized themselves against the martial rule (Philippine Center for Investigative Journalism, 2007). The appointment of women in key government posts followed the accession of the first female president. These developments inspired women’s groups and paved the way for the mainstreaming of women’s rights in the 1987 Constitution. Several landmark laws improving the conditions of women were also enacted. The timely amendment of the Code demonstrated the importance of asserting the government’s prerogative to intervene in matters concerning public health.
Social media provides another platform for the milk companies to flout the law and continue with their promotional activities in cyberspace. Bribing health practitioners veiled as professional development sponsorship is another underhanded tactic of the industry. It is more disturbing to know that industry marketers target the poorest households for their assumed lack of knowledge (Ellis-Petersen, 2018). There is a need for an improved implementation, enforcement, and calibration of the Code to adapt in these dynamic times and the new normal.
Kenneth Jim Joseph Jimeno is a Foreign Service Officer with the Department of Foreign Affairs, in the Philippines.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.