
Diez J, Dharmasaputra T, Ayensu M, Eletta R, Giri A, Medows M. Improving substance use screening among teens utilizing S2BI in a pediatric primary care clinic. HPHR. 2024;74. https://doi.org/10.54111/0001/VVV3
Screening to Brief Intervention (S2BI) is a seven-item validated screening tool for adolescents, used to assess frequency of substance use in the past year. The purpose of this study is to improve substance use screening among adolescents by integrating S2BI in the pediatric primary care clinic.
A quality improvement project was carried out utilizing the Plan-Do-Study-Act (PDSA) methodology. Education was given regarding substance use, screening and intervention strategies. S2BI tools (English and Spanish) were administered to adolescents 12-18 years old before the visit and reviewed with the provider. Ongoing monitoring and feedbacks were obtained, and problems encountered were identified and addressed.
EMR review revealed that 76% of providers failed to ask about substance use. Common reasons were time constraints, forgetting to ask, and clinical impression of no substance use. A total of 228 adolescents, ages 12-18, were screened using S2BI tool in the first 5 months of implementation, with 91% reporting no use. Marijuana (6%) was the most common substance used followed by alcohol (4%) then tobacco (2%). Positive reinforcement was done in 82% of teenagers screened. Addressing barriers increased the monthly screening rate from 16% to 64%. From all the interventions done, incorporation of S2BI tool to the EMR had the greatest impact on the improvement of substance use screening among adolescents in our primary care practice.
In a busy practice, time constraints, knowledge deficits and lack of training may hinder identification of risky substance use. In our clinic, most teenagers reported no use and received positive reinforcement: an indispensable strategy to delay initiation of substance use and prevent its health-related consequences. Even though other interventions were performed at a lesser extent, providers were supplied with patient-centered skills and resources to deal with substance use.
Addressing substance use early in life is crucial to mitigate its effects on the developing brain. Pediatricians, with their long-term relationship with children and their families, play a critical role as first responders to prevent initiation of substance use and its related health and safety consequences. The American Academy Pediatrics (AAP) recommends universal screening for substance use among adolescents and encourages clinicians to follow the Screening, Brief Intervention and Referral to Treatment (SBIRT) model.1 However, research show that many providers fail to screen for substance use or rely on clinical impressions which underestimates teenage substance use.2 Utilizing a brief, validated screening tool provides a statistically tested measure of the level of substance use and can help accommodate the SBIRT model into a busy practice. Screening to Brief Intervention (S2BI) is a seven-item validated screening tool for adolescents, used to assess frequency of substance use in the past year (Figure 1). It has excellent sensitivity and specificity in identifying substance use disorder and can help clinicians select the appropriate specific brief intervention depending on substance use risk stratification.3 In this study, S2BI screening tool was utilized to improve substance use screening among adolescents in the primary care practice.
Figure 1. Screening to Brief Intervention (S2BI) Screening Tool
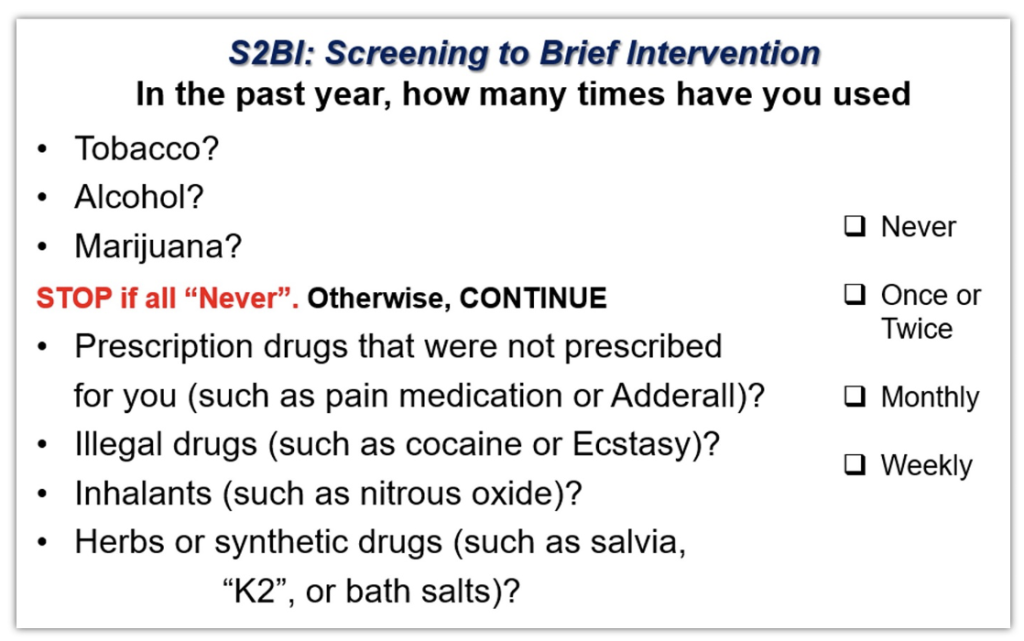
Table 1. S2BI Intervention Algorithm/Pathway
Frequency of Use | Risk Level | Brief Intervention |
Never | No Use | Positive Reinforcement |
Once or Twice | No SUD Risk | Brief Advice |
Monthly Use | Mild/Moderate SUD Risk | Brief motivational intervention |
Weekly Use | Severe SUD Risk | Referral for Treatment |
*SUD – Substance Use Disorder
A resident driven quality improvement project was carried out in a quasi-experimental study utilizing the Plan-Do-Study-Act (PDSA) methodology in a New York City community hospital. PDSA is a useful method which allowed the researchers to test the impact of the quality improvement initiative and continuously improve approach based from experiences. Preintervention survey and electronic medical record (EMR) review were done to determine pediatric providers’ knowledge, perception and practices regarding substance use and screening. Then, education was given regarding substance use in adolescents, importance of screening, use of S2BI tool, brief intervention strategies and resources for referral. Education was given through in-person lectures and individual coaching of pediatric providers. It was supplemented by information packets sent through email and module on motivational interviewing. Motivational interviewing is one of the brief intervention strategies in which providers could use to foster patient motivation to change unhealthy behavior. A pilot study was then performed with 10 providers in a span of 3 months, incorporating S2BI tool at well adolescent visits. Data were obtained from pilot study through survey questionnaire regarding provider experience in S2BI and chart reviews. PDSA cycle was initiated with continuous support provided for the clinicians. A point person was accessible for any questions that clinicians might have when performing S2BI. S2BI screening tools in both English and Spanish were made available (to cater for the Hispanic population which comprises approximately 50% of the patients seen at the clinic) and were administered to adolescents, 12-18 years old, coming in for well child visit at the pediatric primary care clinic. The S2BI screening tools (Figure 1) were handed out to each patient, filled out before the visit and reviewed with the provider. Ongoing feedbacks were obtained and problems encountered were identified and addressed.
A preintervention survey among 34 pediatric providers revealed that 76% failed to ask about substance use in all their adolescent well child visits. Common reasons for not asking were lack of time, forgetting to ask, and impression that the patient does not have risk factor for substance use. On electronic medical record (EMR) review, only 24% of the providers documented that they asked about substance use and no validated screening tools were used. After training and pilot study, S2BI was easily accepted by providers. Ten providers in the pilot study considered that S2BI was brief (less than 1 minute for screening and less than 5 minutes for brief intervention), useful, comprehensive and easy to perform. All of the clinicians agreed that they would continue to use S2BI in their practice.
A total of 228 adolescents, ages 12-18, were screened using S2BI tool in the first 5 months of implementation, with 208 (91%) reporting No Use, 13 (6%) Once or Twice in the past year, 4 (2%) Monthly use and 4 (2%) Weekly use. Marijuana (6%) was the most common substance used followed by alcohol (4%). For the brief intervention, positive reinforcement was done and documented in 186 (82%) of teenagers screened. Positive reinforcement involves a simple statement from the clinician, providing praise towards abstinence from substance use. Brief Advice to stop use was done in 18 patients (8%) while Change Talks which involves motivational interviewing was done in 3 patients (1%). One patient (0.4%) was referred to a specialist (Figure 2).
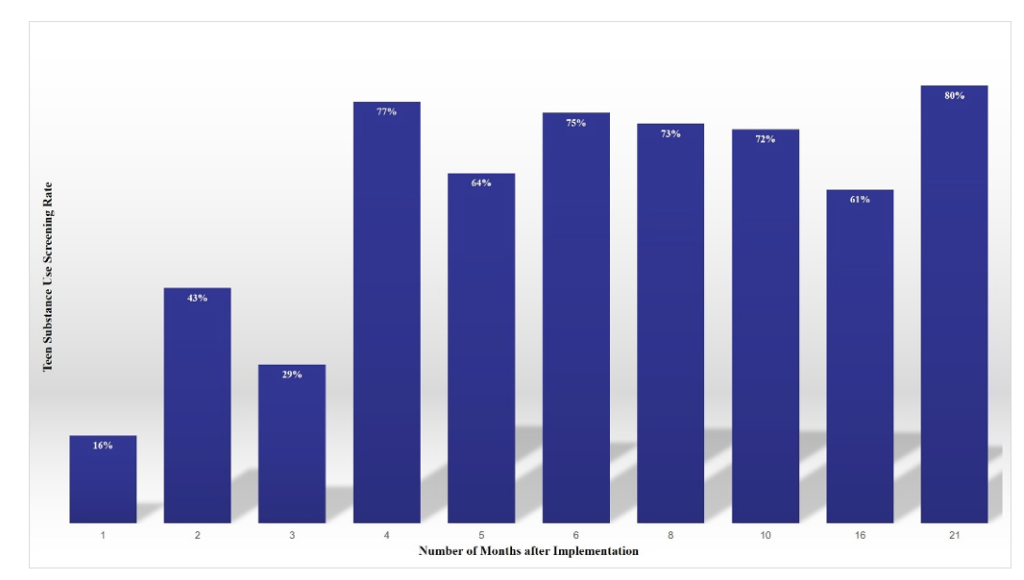
Barriers identified during the implementation were availability of printed screening tools, administration of tool before the encounter, provider recall of screening, knowledge of brief intervention strategies and documentation. Knowledge gaps were addressed through lectures, module on motivational interviewing, messaging application reminders and informative emails. S2BI tool availability and administration were improved through collaboration with the clinical clerks, patient care associates and nurses. Provider recall was improved through incorporation of S2BI to the EMR and placement of S2BI guide in all clinic rooms. Addressing the barriers increased the screening rate from 16% in the first month to 64% in the fifth month (Figure 3). From all the interventions done, incorporation of S2BI tool to the EMR had the greatest impact on the improvement of substance use screening among adolescents in our primary care practice. Continuous monitoring was done and positive change was sustained with a current substance use screening rate of 80% (21 months after implementation).
Figure 2. Results of Adolescent Substance Use Screen and Brief Intervention in the 5-month Implementation period
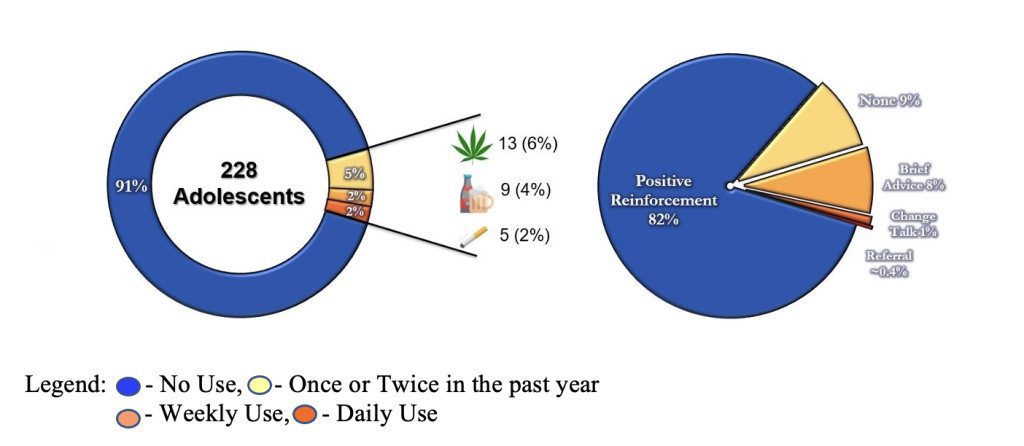
Figure 3. Adolescents Screened with S2BI during the Implementation Period (Month 1 to 5) and Monitoring Period
Adolescence is a time of neurodevelopmental maturation and a period of increased incidence of risk-taking behaviors. This confers them more vulnerable to the detrimental effects of the different substances.4 These includes the effect on brain development, risky behaviors such as unprotected sex and dangerous driving, its contribution to the development of adult health problems such as hypertension and heart disease, and predisposition to substance use disorder in later years.4-5
The American Academy of Pediatrics emphasizes the pediatrician’s role in addressing substance use in adolescents. In the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents screening and anticipatory guidance for substance use were highlighted. Screening whenever adolescents receive medical care increases identification of substance use and opens opportunity for intervention which creates a huge impact in preventing substance-use related health consequences leading to decreased healthcare costs and a more productive years in the future.1
Various validated tools are available to screen for alcohol and other substance use in adolescents. NIAAA Alcohol Screening for Youth,6 a two-item scale to assess alcohol use, is the shortest validated screening tool but is limited to alcohol use. The Screening to Brief Intervention (S2BI),3 The Brief Screener for Tobacco, Alcohol, and Drugs (BSTAD),7 and the CRAFFT8 are all brief screening tools that inquires on past-year frequency of use for different substances. They all have adequate psychometric properties for identifying substance use disorders among adolescents.8-9 However, both BSTAD (11 items) and CRAFFT (9 items) consists of longer questions and thus, entails a longer time to screen. In addition, some of the pediatric providers in our setting were already familiar with S2BI before the implementation, which facilitated ease of use and acceptance.
Screening to Brief Intervention (S2BI), a 7-item screening tool, is efficient in its ability to discriminate among the different degree of substance use disorder (SUD) from no use to severe SUD. S2BI is developed at Boston Children’s Hospital with support from the National Institute on Drug Abuse. It uses a stem question and forced-response options (none, once or twice, monthly, weekly or more) in a sequence to reveal the frequency of past year use of tobacco, alcohol, marijuana and 5 other classes of substances most commonly used by adolescents. Based on the response, patient would be categorized into a specific risk level (No Use, No SUD, Mild/Moderate SUD, Severe SUD) with a corresponding recommended brief intervention. The tool can be self- or interview- administered and is electronic medical record compatible.3
Clinicians in our pediatric clinic found S2BI to be brief, easy to administer, screens for multiple substances, and compatible with electronic medical record. Majority of adolescents screened in our clinic reported no substance use and received positive reinforcement – an indispensable strategy to delay initiation of substance use and prevent its detrimental effects on the developing brain.10 Even though other brief interventions were performed at a lesser extent, SBIRT training for pediatric providers supplied them with patient-centered tools to utilize for various spectrum of substance use. In this quality improvement project, integration of screening tool into the electronic medical record as well as collaboration with other allied healthcare professionals were the integral steps in increasing substance use screening.
Adolescents and young adults are particularly vulnerable for developing substance use disorder due to their developmental and neurophysiological stages.4 However, treatment options for adolescents with substance use disorder are limited. There is also scarcity of addiction specialists especially those trained and comfortable in treating pediatric population.11 Hence, primary and secondary prevention using S2BI or other SBIRT tools are of paramount importance. As shown in this quality improvement project, Screening to Brief Intervention (S2BI) demonstrates great utility in addressing substance use among adolescents which could encourage clinicians to employ this strategy in their primary care practice. In addition, this QI project was performed in an urban community hospital catering mostly the underserved (majority are African-Americans and Hispanics). Increasing capability of pediatric providers in detection and treatment of substance use improves access to care, promotes health equity and reduces health disparities in the population that we serve.
This quality improvement project was performed at a single community hospital serving mostly African Americans and Hispanics. Limited number of adolescents were screened and the results might not apply to other groups. Feedback from pediatricians regarding substance use screening was obtained but there were no feedbacks obtained from patients. Further studies are recommended (e.g. implementation to other hospitals, increasing sample size and diversity of patient included) to improve generalizability of our findings.
This quality improvement project was performed at a single community hospital serving mostly African Americans and Hispanics. Limited number of adolescents were screened and the results might not apply to other groups. Feedback from pediatricians regarding substance use screening was obtained but there were no feedbacks obtained from patients. Further studies are recommended (e.g. implementation to other hospitals, increasing sample size and diversity of patient included) to improve generalizability of our findings.
Screening to Brief Intervention (S2BI) screening tool was proven to be concise and useful in identifying substance use among adolescents in a busy primary care clinic. Time constraints and knowledge deficits could hinder substance use screening and was addressed through education, integration of tool in the electronic medical record, and collaboration with allied healthcare professionals. Most of the teens screened in our practice reported no substance use and received positive reinforcement, which is a valuable strategy in delaying substance use.
The authors have no relevant financial disclosures or conflicts of interest.
We would like to thank all the pediatricians, residents, and nurses of Woodhull Hospital Department of Pediatrics for their dedication in caring for our patients.
Dr. John Robyn Diez is a chief resident of the Department of Pediatrics, Woodhull Medical and Mental Health Center (NYU Affiliate). He received his nursing and medical degree in the Philippines. Before pursuing his career in the United States, Dr. Diez has completed pediatric training in the Philippines in an urban hospital catering mostly the underserved. He is particularly interested in research and quality improvement projects tackling the prevention and treatment of substance use disorder in the youth.
Dr. Dharmasaputra is a 3rd year pediatric resident at Woodhull Medical and Mental Health Center. She received her medical degree in Indonesia.
Dr. Ayensu is a 3rd year pediatric resident at Woodhull Medical and Mental Health Center. She received her medical degree in Ghana.
Dr. Eletta is a pediatric chief resident at Woodhull Medical and Mental Health Center. She received her medical degree in Nigeria.
Dr. Giri is a 3rd year pediatric resident at Woodhull Medical and Mental Health Center. He received his medical degree in Nepal
Dr. Medows is the current Associate Pediatric Residency Program Director at Woodhull Medical and Mental Health Center. She is also an Associate Professor in Pediatrics at NYU Grossman School of Medicine. She is a board-certified pediatrician and pediatric hospitalist.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.