
Tillewein H, Toufik A, Awuah W, Zuñiga Y, Shellah D, Colescu A, Carpenter C, Le Compte C. Legislating the new Gilead: implications of the Texas Heartbeat Act. HPHR. 2022;56.10.54111/0001/DDD2
On September 1, 2021, the state of Texas passed a new law, Texas SB8 or the Texas Heartbeat Act that effectively allowed a near-total ban on abortion. The law prohibits all abortion after 6 weeks gestation, with no exceptions for rape or incest. Supporters champion the legislation as a landmark in protecting the life of the unborn, without referring the stark repercussions SB8 will have for women, girls, and other persons with a uterus. While the most extensive, the Texas Heartbeat Act marks one numerous bills in states across the U.S. that seek to limit access to sexual and reproductive health services. These bills disproportionately impact those with a uterus from medically underserved populations, including racial and ethnic minorities, LGBTQIA+ persons, rural dwellers, and those experiencing poverty and housing instability. Without legal protections, persons seeking abortions face social stigmatization and violence, medical mistreatment, and possible criminal prosecution. As public health professionals, we must ensure that abortions remain a viable part of reproductive health.
Access to safe abortion, the intentional termination of a pregnancy via surgery or medicinal means, is essential to women’s bodily autonomy and optimal health outcomes. Between 1973 and 2022, this right was guaranteed by the Supreme Court decision, Roe v. Wade. The original decision reflected the need to provide safe access to the procedure, which was commonly done in risky settings.1–8 Without medical intervention, abortion can result in high rates of injury and death.9–12 Prior to 1973, women of financial means were able to access to abortion from doctors willing to provide the procedure or travel to countries where it is legal. Other women suffered; many women who died from illegal abortions during that time period were Black and/or low socioeconomic status who self-induce at 12 weeks or beyond out of desperation. After passage of Roe v. Wade decision, deaths from illegal abortions decreased from 39% to 5%.3 From 2015-2019, the rate of unintended pregnancy rate in Europe and North America was about 3.5%. Close to one-half (49%) of these pregnancies ended in abortion.13 In 2019, there were an estimated 629,898 legal abortions in the U.S., which translates to 11.3 per 1,000 pregnancies.14 Of these abortions, 92.2% were performed at less than 13 weeks’ gestation; so-called late term abortions were much less frequent, with 6.9% performed at 14-20 weeks’ gestation, and 1.0% performed later than 21 weeks’ gestation.15
While a relatively rare procedure, abortion access is heavily contested in the U.S. Conservative forces have sought to overturn Roe v. Wade since its passage. Champions of women’s health care have called the undermining of Roe v. Wade as a slippery slope toward the establishment of real-world Gilead, the Fascist regime of Margaret Atwood’s 1985 novel, The Handmaid’s Tale. Gilead in the novel overthrows the U.S. Federal government, disenfranchising women and creating a class of gestational slaves called handmaids.16 While still somewhat removed from Atwood’s dystopian landscape, Roe v. Wade was steadily undermined until its reversal in June 2022. Texas’s SB8 or Texas Heartbeat Act, passed just 10 months prior, in September 1, 2021, provided a template to overthrow Roe v. Wade, legalizing a near-total ban on abortion. The law prohibited abortion after 6 weeks, strengthening measures Texas already has in place to limit abortion based on gestational age, the number of weeks after a women’s last known period or conception.17
Prior to SB8, limits on abortion access were increasingly common in the U.S; 43 other states had laws in place to limit abortion based on either gestational age or fetal viability, defined as fetal development that enables life outside the uterus under normal conditions.17 SB8, however, stood apart as one of the most restrictive laws on the books. The 6-week time span was 22 weeks shorter on average that other laws that use gestational age and allows no exceptions for pregnancies conceived through rape and incest or that endanger the patient’s life or health.18 It also provided no exceptions for rape or incest,38 and established legal provisions that enabled citizens to enforce the law.19
Supporters have cast the Texas Heartbeat Bill as a fair compromise for patients and abortion providers, since it allows abortions for the first six weeks of pregnancy. Most women, however, do not know they are even pregnant until 5.5 weeks,1 with nearly one-fourth (23%) of women not learning they are pregnant until much later.2 As such, the law already has diminished access to safe and legal abortions and reproductive services, with the few remaining abortion providers in the state able to provide appointments to those who need them.1
In addition to its sweeping restrictions, Texas Heartbeat Bill remains singular in casting individual citizens as agents of the state, penalizing those seeking abortions or facilitating their access (whether a medical provider or a rideshare driver transporting a patient to an abortion appointments), through $10,000 lawsuits.5 The atmosphere of vigilantism already has created a threatening and unsafe environment for pregnant persons seeking abortion care, and discouraged medical professionals from providing reproductive services. Since SB8’s passage, a former lawyer and convicted felon from Arkansas file a private lawsuit against a Texas doctor who performed an abortion on a woman past the legal gestational period.6
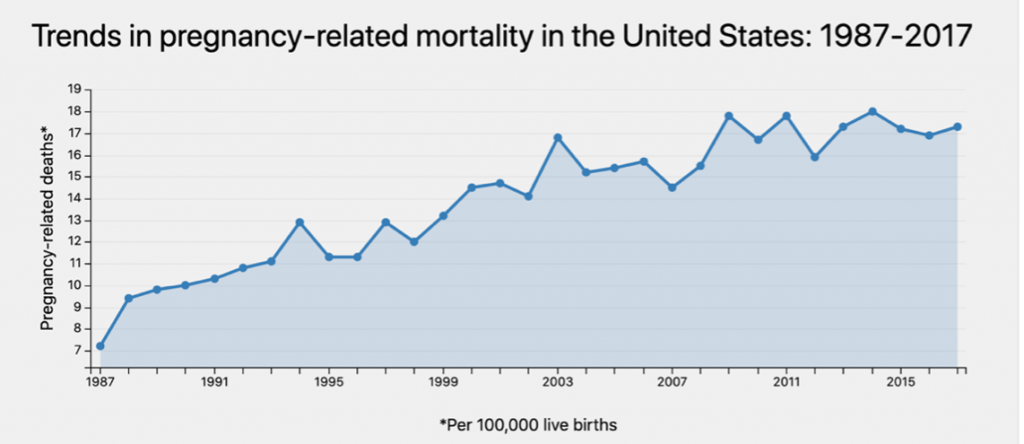
Though cast as protective of children, restrictive abortion laws actually contribute to maternal and child death. Indeed, research has shown that states with strict gestational limits on abortion access typically have the highest maternal mortality rates in the U.S.14 and an excess infant deaths.20 States that have limited abortion provision typically report maternal deaths per 100,000 births significantly higher than the national average: Texas (34.5 per 100,000 births) Arkansas (45.9 per 100,000 births), Alabama (36.4 per 10,000 births), Kentucky (40.8 per 100,000 births), and Ohio (30.1 per 100,000 births).21 By contrast, a systematic review of 162 ecological studies has shown that flexibilities in legal instruments such as abortion law are associated with lower maternal mortality rates.22 Hence, legal instruments like progressive abortion laws can ensure quality and timely access to services.
Maternal and child mortality disproportionately impacts communities of color, notably Black, Hispanics, and Native Americans. Most significantly, the Texas Heartbeat law will have a monumental impact on women of color, and female survivors of sexual assault. In 2014, about 75% of abortion patients were low income. These groups on average face the greatest difficulty accessing safe abortions due to limited access to high quality reproductive care, financial obstacles, geographic impediments, lack of access to timely abortions, and lack of access to safe abortions. Additionally, gestational limits, coupled with threats against abortion providers and laws that target abortion facilities, often force women to consider options farther from home or consider less safe options, such as untrained providers or pills unknown origin and limited directions for uses. The confusion and increases in travel, time, emotion, and financial costs often create insurmountable barriers that force 85% of women in these circumstances to forgo the procedure altogether.7
Stringent abortion policies encourage the delivery of infants by mothers who are unable to support an infant economically or emotionally. Furthermore, lower socioeconomic women may experience limited access to prenatal care and healthcare for the child, which further exacerbates adverse effects on maternal and infant health.7 Unless these women have the resources to travel, SB8 forces pregnant persons who want an abortion to remain pregnant against their will; women pregnant due to violence (rape), sexual abuse, or incest, or experiencing a fetal anomaly will be forced to give birth.19,23 These unwanted pregnancies in Texas are much more likely to have occurred among low-income women already experiencing food insecurity and housing instability, and transportation.23 SB8 has increased the risk that those forced to give birth would have ongoing contact with an abusive partner or assailant, resulting in costs of court cases to settle custody issues. The community also will bear increased strain on local foster care systems, while women who experience still birth or give birth to babies with life-limiting anomalies will have to bear increased medical and health insurance costs.23
Carrying an unwanted pregnancy can be psychologically damaging, especially women who conceive through rape or incest. The odds of this occurring are high. The CDC reports that 1 in 3 women will experience sexual violence during their lifetime,24 and an estimated 3 million women will experience rape-related pregnancy.18 Women who report such pregnancies often are raped by an intimate partner (26%) who may already have been engaged in reproductive coercion (forcing a partner to get pregnant) by blocking access to birth control pills (20%) or barrier methods (23%).24 States with the highest rates of rape, including Alaska (148.7 per 100,000 inhabitants), Arkansas (77.2 per 100,000 inhabitants), South Dakota (72.6 per 100,000 inhabitants), and Michigan (72.4 per 100,000 inhabitants),25 are among those with the strictest abortion laws, limiting use of telemedicine to administer medication abortion, requiring parental consent for minors seeking an abortion, and instating state-directed counseling that includes information discouraging the use of abortion.26 Texas’ statute stands out for requiring persons who conceive babies through rape or incest to term, rape victims possibly facilitating child visitation with their rapist.
Heartbeat Bills may be useful tools to reduce the prevalence of abortions; however, such tools may pose more harm than good to women by preventing safe, accessible, and affordable abortions, increasing maternal mortality rates and undermining freedom of choice and rights to reproductive health for women. Women also will have an increased risk of poorer mental and physical health throughout their course of life due to the shaming and proverbial policing of abortion.18 Moreover, the Texas Heartbeat bill stigmatizes women and disproportionately impacts women of color, immigrant women, and women with disabilities.
Public health professionals need to advocate for equity in reproductive health for all women. As public health professionals, we need to educate legislatures and government officials on the importance of providing safe abortions for women and ensure continued access to safe abortion through multiple means, whether in person or through delivery of medications, especially now that Roe v. Wade has been overturned.
Figure 1: State-by-State Abortion Laws in the U.S.27
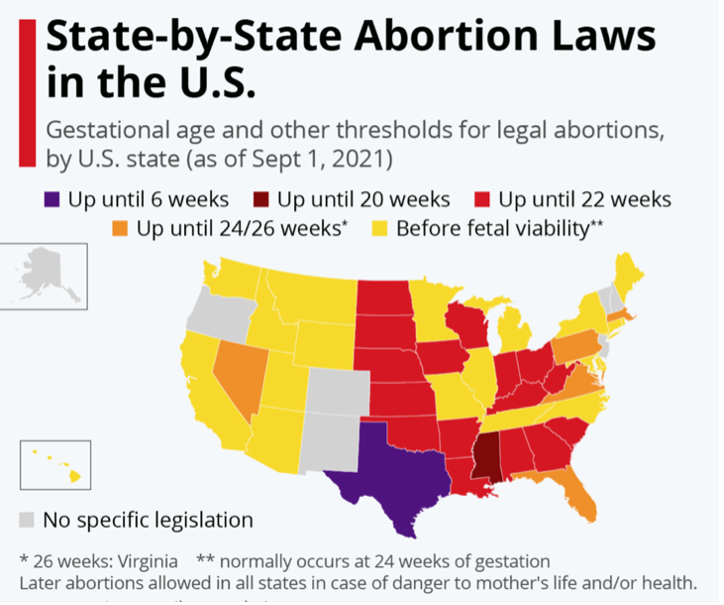
Figure 2: Trends in Pregnancy-Related Mortality in the United States: 1987-20174
The author(s) have no relevant financial disclosures or conflicts of interest.
This research received no specific grant from any funding from any agency. Ethical approval was not required on account of no
study participants.
Heather Tillewein, PhD, CHES, is an Assistant Professor of Public Health at Austin Peay State University. Dr. Tillewein is on the Executive Committee, Policy Committee, and serves as Communication’s Chair for the LGBTQ Health Caucus for the American Public Health Association. She also serves as Director for Special Editions and Associate Editor for the HPHR Journal. Dr. Tillewein’s current research focuses on LGBTQIA+ health, sexual health, and mental health.
Abdul-Rahman Toufik is a medical student at Sumy State University, Ukraine with a diploma in International Environmental Law and Governance with the “United Nations Environmental Law and Conventions”. He is the CEO and founder of Toufik’s World Organization and Toufik’s World Medical Association. He is also an Associate Editor at the Harvard Public Health Review and The Nyc Daily Post. Due to his passion for diplomacy and research works he has participated and also held several International Positions on various United Nations and medical conference platforms.
Wireko Andrew Awuah is a Ghanaian who lives and schools in Ukraine. he holds a Diploma in International Law and Global Governance with the International Business Management Institute, Berlin, Germany. He is a Diplomat who holds several International positions on various United Nations platforms. He is currently serving as an Editorial Board Member of the HPHR Journal, and 4 other reputable journals in the UK, Canada and India. He serves as an ambassador for over 15 European and UK medical conferences and over 10 other reputable social networks. A proud winner of great international awards like the Young Scientist Award 2021.
Yves Miel H. Zuñiga is the Co-Founder and Deputy Director for Policy and Partnership of MentalHealthPH in the Philippines. As an independent public health consultant, he works in the areas of non-communicable diseases, health policy, and health systems strengthening.
Duha Shellah is the chief executive officer (CEO) & Founder of the research community of Palestine “The Researchist”. She is an Elsevier Student Ambassador. Duha is a Student Editor & Palestine Ambassador at the International Journal of Medical Students. She has been assigned as an Associate Editor and Director of Recruitment HPHR Journal (Formerly Harvard Public Health Review). Also, Duha is Country Coordinator at the International Youth Alliance for Family planning (IYAFP). She is intern writer at In-Training Magazine. Newly, She got the membership of Committee of Publications Ethics (COPE). Also, Duha is the General Secretary of Toufik’s World Medical Association. Duha is an MD candidate, studying at An-Najah National University, Palestine Nationally, Duha, is an ambassador for the Palestinian Forum for medical Research and the third undergraduate Research conference – Al Quds University. Duha is a founder member in Palestinian women in surgery community in Palestine.
Alice Colescu is a 3rd year medical student from Romania, Europe. She serves as a Managing Editor for the HPHR Journal, an Assistant to the Co-Editor-in-Chiefs of the HPHR Journal, as well as a Managing Editor for Toufik’s World Organization Journal. Alice is a local Officer of Research Exchange and PR Coordinator of Walter Dandy Neurosurgery Club.
Candice Danielle Carpenter, MD, MBA, MPH, EdM. Dr. Carpenter serves as Co-Editor-in-Chief of HPHR Journal, and is Founder and Co-CEO of The Boston Public Congress of Public Health. She is also Executive Producer of the Great Health Debates. She is a neurosurgeon-in-training, bio and social entrepreneur, educator, and social justice advocate.
Circe Gray Le Compte, ScD, SM serves as Co-Editor-in-Chief of HPHR Journal, and is Founder and Co-CEO of The Boston Public Congress of Public Health.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.