
Rea S. Chen W. Ikoma M. Szakasits L. Young J. Disproportionate suicidality in LGBTQ+ youth in the United States through the socioecological. framework. HPHR. 2021;42.10.54111/0001/PP3
The aim of this paper was 1) to evaluate contributing factors to high suicidality rates among LGBTQ+ youth, and 2) to explore options for interventions to improve mental health and reduce suicidality among LGBTQ+ youth.
Suicide is the second leading cause of death in the United States (U.S.) among those age 10-24, and rates have increased significantly over the past decade. The burden of suicidality, including suicidal ideation, plans, and attempts in U.S. youth is disproportionately shared by lesbian, gay, bisexual, transgender, and queer (LGBTQ+) youth, with U.S. high schoolers who identify as lesbian, gay, or bisexual being nearly four times as likely as their heterosexual peers to attempt suicide. Opportunities to address disproportionate suicidality in LGBTQ+ youth exist at several levels.
Various social determinants of health contribute to disproportionate rates of suicidality for LGBTQ+ youth in the U.S., including national and state policy, income and housing discrepancies, social support in schools and homes, and access to nondiscriminatory health care. As determined by a causal loop diagram and supported by a socioecological framework, increasing access to health care through means such as telehealth services and developing cultural competency programs aimed at reducing stigma is vital. In addition, involving families, teachers, and peers of LGBTQ+ youth will be critical in building and strengthening existing school-based programs to enhance support and belonging for LGBTQ+ youth.
Suicide is the second leading cause of death in the United States (U.S.) among those age 10-24.1 Over the past decade, suicide rates have nearly tripled in youth age 10-14 and increased 76% in those age 15-19.2 Moreover, the burden of suicidality—which encompasses suicidal ideation, plans, and attempts—among U.S. youth is disproportionately shared by those who identify as lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ+) and has been steadily increasing among U.S. youth since 2009.3
Suicide has devastating short-term and long-term consequences on those affected, their support networks, and the health care system. Accounting for direct medical costs and indirect costs such as lost productivity, the average cost of one suicide among those 15-24 years old is estimated to be $2,012,476.4 The intersection of adolescent development and disparities within the LGBTQ+ community create a significantly elevated risk for both mental illness and suicide. Sixty percent of adolescents diagnosed with major depressive disorder (MDD) report having suicidal thoughts and 30% of these adolescents actually attempt suicide.5 Additional risk factors for suicide attempt include prior suicidal behavior, substance use, and identification as LGBTQ+.6 In 2019, nearly half (47%) of LGB students reported “seriously considered attempting suicide” in the preceding 12 months compared to 15% of their heterosexual counterparts.7 U.S. high schoolers who identify as lesbian, gay, or bisexual were nearly four times as likely as their heterosexual peers to attempt suicide in 2019 (23.4% versus 6.3%), and half of all transgender youth report having at least one previous suicide attempt.7,8
The causes of the alarming increase in adolescent suicidality demand investigation, particularly within the LGBTQ+ population. Many social determinants of health have been implicated in the disproportionately poor mental health outcomes for LGBTQ+ youth. These determinants include national and state policy, income and housing discrepancies, strength of social support in schools and homes, access to nondiscriminatory health care, and biological factors. The aim of this paper was 1) to evaluate contributing factors to high suicidality rates among LGBTQ+ youth through a socioecological framework (Figure 1), and 2) to explore options for interventions to improve mental health and reduce suicidality among LGBTQ+ youth.
A complex interplay of social, political, and economic structures permit the systematic suppression and discrimination of LGBTQ+ individuals, consistent with factors found within the regional, national, and global systems of our socioecological framework (Figure 1). This leads to elevated levels of psychological distress. Much of the literature reveals that LGBTQ+ individuals are more likely to be poor than their heterosexual and cisgender peers. Poverty particularly affects youth, and in 2018, the U.S. Census Bureau reported that 16% of people under the age of 18 lived below the poverty line compared with 11% of adults aged 18-64.9
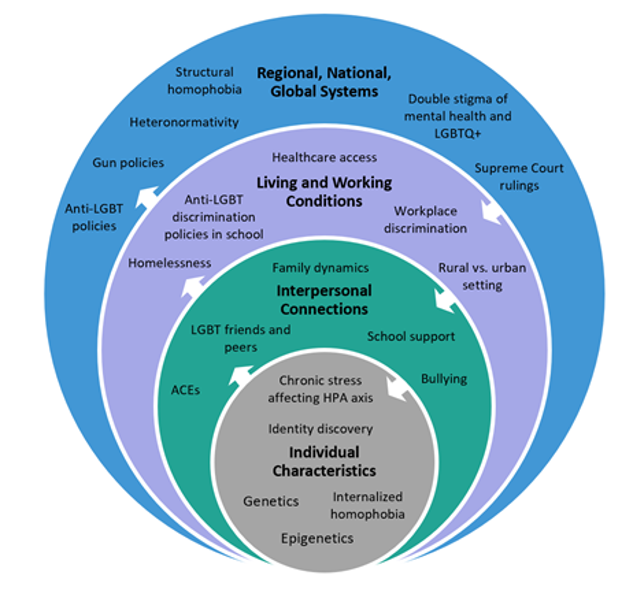
Figure 1: Socioecological Framework for LGBTQ+ Youth Suicidality
Income rates impact the ability to afford housing, and this coupled with lack of social support, is another economic factor that influences psychological well-being. LGBTQ+ youth are more likely to experience homelessness, accounting for 20-40% of the homeless population despite making up less than 3% of the total U.S. population.10,11 Running away from home, being thrown out by their families, and placement in foster homes drives this elevated rate.10,12 Homeless LGBTQ+ youth—particularly transgender individuals—are more likely to be physically and sexually assaulted, and they experience rates of sexual assault three times higher than non-LGBTQ+ homeless youth.10 LGBTQ+ youth often face difficulties accessing shelters, which can be a site of vulnerability and danger due to lack of private showers, discrimination from shelter staff, and even outright denial of admission.10 The lack of stable housing results in increased risk of victimization and negative health outcomes, including greater likelihood of suicidal ideation.12
Prior to the U.S. Supreme Court ruling in 2015 legalizing same-sex marriage, individual states either banned or permitted same-sex marriage, and this political factor contributed strongly to the psychological distress among members of the LGBTQ+ community. Of the 32 states that implemented policies permitting same-sex marriage prior to 2015, there was a significant relative reduction (14%) in suicide attempts among youth aged 15-24 compared to states that did not.13 The link between political acceptance and mental health outcomes is further buttressed by the increased prevalence of mental health disorders in states that banned same-sex marriage.13
Behavioral and psychosocial determinants, identified within the interpersonal level of the socioecological framework, shape the mental health and risk of suicidality in LGBTQ+ youth. The Minority Stress Model explains how stressors disproportionately affect social minority groups. Minority stress experienced by LGB individuals includes acute and chronic events and conditions, anxiety associated with anticipation of these stressful events, and the internalization of negative societal attitudes.14 The internalization of prejudice and discrimination from a youth’s family, peers at school, or greater societal bias can increase the risk of depression, which can then evolve into suicidal ideation and behaviors.15
There are also racial disparities in family acceptance and rejection that create a complicated intersection between youth development, sexuality, family relationships, and mental health risks. Richter and colleagues found that Hispanic, Latino, Black, and multiethnic parents were more likely to report rejection and homonegativity toward their LGB adolescents than white, non-Hispanic parents.16 Youth who identify as both LGBTQ+ and as a person of color are likely to experience compounded discrimination, prejudice, and systemic bias that contributes to poor mental health outcomes.
Another psychosocial determinant of mental health outcomes for LGBTQ+ youth is the school environment. Friedman and colleagues found that LGB youth were 2.4 times as likely to miss school out of fear of peer victimization as their heterosexual classmates.17 A mixed-methods study of 13-25 year old LGBT youth in England found that of participants who self-harmed or felt suicidal, 89% reported that their distress was attributed to problems with friends, bullying, or family dynamics.18 McDermott and colleagues found through interviews that determinants of suicidality included homophobia and bullying, sexual and gender norms, managing or hiding their identities in various settings, and life crises related to lack of social support groups.18 Bullying of LGBTQ+ youth places them at an increased risk of poor mental and physical health, including depression, worse quality of life and self-worth, substance use, sleeping difficulties, greater BMI, and higher blood pressure than youth who are not bullied.19
Adverse childhood experiences (ACEs) include physical and sexual abuse, neglect, and household dysfunction, which lead to worse mental health outcomes in adulthood. A meta-analysis of 26 school-based studies in 2011 concluded that LGB youth are 1.7 times as likely to be physically threatened, injured, or assaulted, 1.2 times more likely to experience physical parental abuse, and 3.8 times as likely to experience childhood sexual abuse.17 These experiences can all be categorized as ACEs which significantly interfere with youth development. According to Clements-Nolle and colleagues, LGB youth in grades 9-12 were more likely to have higher individual and cumulative ACEs than heterosexual students.20 This study examined the YRBS data from grades 9-12 in Nevada and found that LGB youth with 2 or more ACE’s had approximately a 13 times higher odds of suicide ideation and attempts.20 This alarming relationship between ACEs and suicidality, especially for LGBTQ+ youth, must be studied more closely to apply appropriate screening and interventions.
Environmental factors play a role in the disparity of suicide rates in the LGBTQ+ youth population, as noted in living and working conditions in the socioecological framework. The most pertinent environmental factors include geographical location and access to local nondiscriminatory health care resources. It is estimated that roughly 10% of youth in the U.S. identify as LGBT, with rural and urban youth identifying as LGBT at equal rates.21 Rural states are less likely to have laws that protect LGBT youth.21 For example, only 31% of rural states have LGBT-inclusive anti-bullying school laws compared to 53% of urban states.21 Additionally, conversion therapy, an outdated and discredited attempt to change someone’s sexual orientation or gender identity, has been shown to significantly increase risk of depression and suicide attempts among youth; yet, only 13% of rural states have conversion therapy bans compared to 63% of urban states.21 Several studies have also shown that rural counties tend to have 1.8 times higher suicide rates than urban counties, most commonly attributed to access to firearms.22–24
Proximity to adequate health care is another important environmental factor. In a 2020 Executive Summary by the Trevor Project, more than half of LGBTQ+ youth who reported wanting mental health care in the past year did not receive it, citing reasons including inability to afford care, lack of transportation to get to a clinic, or the nearest facility being too far away.25 LGBT people in rural areas have even less access to LGBT-specific services, with only 11% of LGBT people in rural areas having access to an LGBT health center compared to 57% in urban areas.26
A significant source of inadequate medical care stems from the stigma and victimization that the youth LGBTQ+ population faces, which leads to chronic stress. This stigma and stress is identified at the individual level of the socioecological framework, but bias also extends throughout all levels. Studies have repeatedly shown that LGBTQ+ youth are more likely to experience stigma compared to heterosexual peers, including in health care settings.27 This serves as a precursor to adverse psychosocial outcomes, primarily depression and suicide. It has been shown that certain social factors, such as anticipated negative responses to gender identity and behavior, conflicts and concern regarding disclosure of sexual orientation to providers, and mistreatment in community settings lead to mistrust and lack of follow up with health care providers.28
Implicit biases about LGBTQ+ people can negatively impact care. Formal education and training on healthcare for LGBTQ+ people is not traditionally offered in most medical educational curricula. This lack of training can lead to gaps in medical care and causes missed opportunities to address the medical and psychological needs of this population. In 2013, the American Academy of Pediatrics released a statement urging all pediatricians to provide culturally effective care to help reduce disparities among the LGBTQ+ population.29 A 2016 study of over 4000 first year heterosexual medical students revealed that half of these participants exhibited forms of explicit biases towards LGBTQ+ people and over 80% of participants exhibited forms of implicit biases.30
Biases among health care providers lead to poorer health outcomes and quality of services for LGBTQ+ people.31 A 2015 systematic review of medical education curricula showed that programs that included training and education on LGBTQ+ bias overall showed a promising reduction of bias among health care professional students.31 Bias, whether explicit or implicit, can cause inadequate screening and medical care needed to help close health disparities and can serve as a detrimental cause of poor outcomes for the LGBTQ+ community.
Based on findings from the sections above, a causal loop diagram was created, and determinants that contribute to suicidality in LGBTQ+ youth and their interactions were identified (Figure 2). Discrimination of LGBTQ+ youth, shown at the left of the diagram, is a common upstream determinant of many other factors leading to suicidality. Discrimination is positively associated with poor health care access, mental health problems, and inadequate family and school support, all of which have a complex interplay with each other. Specific health needs of LGBTQ+ youth are often excluded in medical training, and providers and clinic support staff may not be inclusive or use unbiased language with patients or on intake forms. This creates a barrier to accessing non-discriminatory, regular health care, which then contributes to mental health problems. Poor family support for LGBTQ+ youth also contributes to a significantly increased risk of suicidality. Lack of social support prevents youth from having regular health care through limitations of confidentiality and privacy related to being out or insurance coverage through parents, transportation barriers, or lack of inclusive health resources at schools. Chronic stress from inadequate family support contributes to youth suicidality, as does bullying, lack of peer and teacher support, and heteronormativity of most sexual education programs in school. From this diagram, health care access and school-based support were targeted as priorities for intervention and are described below.
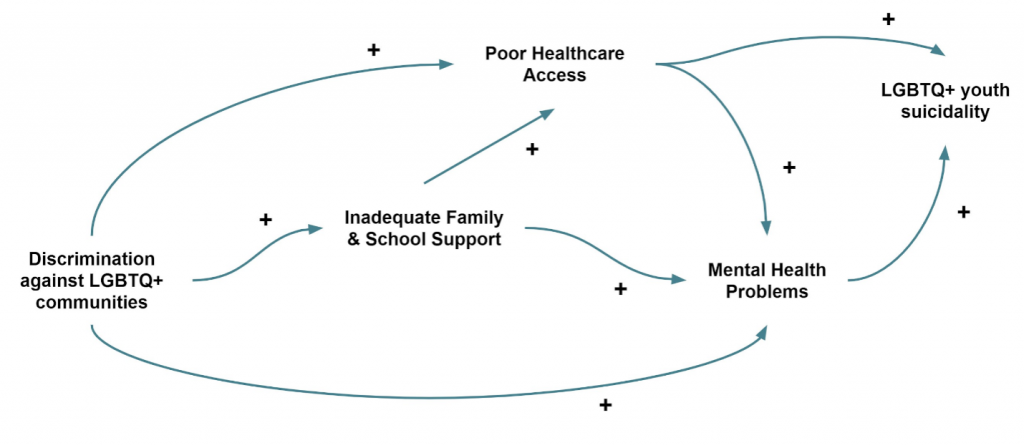
Figure 2: Causal Loop Diagram: Determinants Associated with Suicidality in LGBTQ+ Youth
Lack of healthcare access plays a major role when exploring upstream factors contributing to mental health disparities among the LGBTQ+ population and should be a priority for interventions to decrease suicidality rates. Telehealth has the potential to address both challenges secondary to rural living and access to available providers who have training in LGBTQ+-specific issues. Telehealth allows the patient to connect with an appropriate provider and receive the same mental health evaluation as one would in an office setting. In addition, many LGBTQ+ youth feel more comfortable with disclosing personal and sensitive information to a new provider virtually.25 Telehealth can also eliminate transportation difficulties that would limit one to obtain care. Although there are limited studies in the United States that examine the benefit of telehealth and mental health outcomes in LGBTQ+ youth, telehealth has been proven to be beneficial in other aspects of adolescent and young adult psychiatric care.32
Another potential intervention is increasing LGBTQ+ cultural competency among health care providers. As discussed above, stigma is a significant source of psychiatric outcomes. Implementing educational programs on cultural aspects of the LGBTQ+ community and important aspects of their care may increase access by decreasing stigma and increasing patient comfort, satisfaction, and trust. Data examining the effects of such training on overall patient outcomes is lacking, but many studies assessing these models demonstrate that providers who receive cultural competency training feel more confident and competent when caring for LGBTQ+ patients. One example is the Curriculum for Oncologists on LGBT populations to Optimize Relevance and Skills (COLORS) training curriculum, an interactive educational program used to increase LGBTQ+ cultural competency among oncologists.33
The framework of community-based participatory research (CBPR) can aid in ensuring community engagement by improving communication between the TGD and research communities.24 CBPR emphasizes community stakeholders as equal partners working in collaboration with researchers. The expansion of CBPR in TGD health research by including TGD community members in the research process will help researchers to address evolving language, reduce bias, and build trust.
In addition to promoting community engagement through CBPR, we must focus greater investment in clinical research projects focusing on TGD health. Although calls continue for more clinical research focusing on sexual and gender minorities, institutional and financial support present major barriers for researchers.25 Funding for clinical research must increase for all sexual and gender minorities, but allowing researchers dedicated grants to focus in particular on the paucity of comprehensive longitudinal clinical research for the TGD population will have a significant impact on developing future guidelines for clinicians of all specialties.
To address inadequate family and peer support, which contributes to a significantly increased risk of suicidality among LGBTQ+ youth, interventions must target home and school environments. Bullying and harassment have been shown to lead to chronic stress and mental health problems, which could be addressed with stronger implementation of anti-bullying policies in schools.34 While anti-bullying policies have been passed in all 50 states, the limitations of enforcement include not having enough staff to investigate reports of bullying, differences in definitions of consequences for those who bully, and language confusion surrounding harassment, peer aggression, and bullying.35 Additionally, most policies are not specific to LGBTQ+ youth, which prevents explicit protection of this population. The shortcomings of these policies create a goal of implementing effective prevention strategies.
Prevention of harassment and bullying includes Gender-Sexuality Alliance (GSA) programs in schools. A study of approximately 20,000 students found that schools with GSA’s and anti-bullying policies that were specific to LGBTQ+ youth decreased both discrimination and suicidality.36 Schools that implemented these programs 3 or more years ago had stronger results, indicating that establishment of these programs as a norm is beneficial to LGBTQ+ youth. A meta-analysis of more than 60,000 students found that GSA’s were associated with less victimization, reduced fear of safety, and decreased verbal harassment.37 Additionally, schools that teach LGBTQ+ health and encourage staff training for LGBTQ+ inclusion and anti-bias demonstrated fewer suicidal thoughts in their LGBTQ+ students.15 By creating school environments that consistently foster inclusion, education, safety, and prevention, youth LGBTQ+ suicidality will decrease.
Research on LGBTQ+ mental health and successful interventions to decrease suicidality rates is limited and dated. The paucity of research is likely due in part to the lack of the inclusion of sexual orientation and gender identity questions in national surveys and research studies. Although the Healthy People 2010 Initiative had identified the need for more national surveys to collect sexual orientation data, only two national data collection systems have added sexual orientation to their surveys in the past decade.38 The CDC’s YRBS is one of the most prominent survey systems that collects data on youth and suicidality, but does not require sexual orientation questions on their surveys. Thus, some of the data in this paper was obtained from nonprofit organizations such as the Trevor Project and GLSEN (Gay, Lesbian & Straight Education Network) that independently collected data and published reports on their websites, which might not have been peer-reviewed to the same standard as articles published in academic journals or by governmental agencies.
There is a clear need for data, both qualitative and quantitative, in LGBTQ+ youth not only for better understanding the determinants contributing to their health inequities and disproportionately high suicidality rates, but also for designing and properly assessing interventions. Specifically, more research is needed on the intersectionality of factors influencing LGBTQ+ suicidality, including race and ethnicity and familial socioeconomic status. Since most of the past research has been done exclusively on LGB individuals, expanding the data on transgender, queer, questioning, pansexual, asexual, and intersex individuals is also necessary. Additionally, in a study examining NIH-funded research from 1989 to 2011, only 202 studies were found to examine LGBT health-related interventions.39 This scarcity over 22 years is evidence that more randomized control trials or longitudinal studies are needed, and these intervention studies need to take into account the effects and outcomes on LGBTQ+ community members.
Elevated rates of suicide among LGBTQ+ youth in the United States are driven by systematic oppression and discrimination. Institutionalized homophobia and stigma lead to a lack of social support and poor access to health care and are currently the most significant drivers of morbidity and mortality within the LGBTQ+ community. LGBTQ+ youth are particularly vulnerable to these factors because they face harassment both by peers within school and by family at home, and oftentimes access to life-saving health care is limited due to discrimination and dependency upon these social supports. Policies aimed at reducing stigma and rejection within family systems are difficult to enact. However, policies targeting both school support and adequate access to mental health care are possible, enforceable, and would provide the greatest benefit in reducing suicidality rates among LGBTQ+ youth.
We would like to thank Dr. Jon Hussey for his support and editing of this manuscript.
The author(s) have no relevant financial disclosures or conflicts of interest.
Samantha Rea is a MD student at the Wayne State University School of Medicine. She completed her MPH at University of North Carolina at Chapel Hill. She is pursuing a residency in pediatrics and pediatric physical medicine and rehabilitation. Her interests include health policy, social determinants of health, and adolescent sexual and reproductive health.
Willa Chen is a fourth-year medical student at the UNC School of Medicine applying into family medicine this year. They received her their MPH at the UNC Gillings School of Global Public Health. Their interests include full-spectrum family medicine, LGBTQ+ health, mental health, global health, and health disparities.
Jessica Young, MD is a pediatrician from rural eastern North Carolina. She is currently training in Preventive Medicine at UNC Chapel Hill. Her clinical and research interests include adolescent reproductive health, childhood obesity, health disparities, and quality improvement in primary care.
Michelle Ikoma is a fourth-year medical student at the UNC School of Medicine. She completed her MPH at the UNC Gillings School of Global Public Health. She is passionate about the intersection of physical and mental health and is pursuing combined residency training in family medicine-psychiatry. Her professional interests include primary care mental health integration, adolescent medicine, LGBTQ+ health, medical education, and clinician well-being
Lindsey Szakasits completed her MD/MPH training at the University of North Carolina at Chapel Hill and is now completing a psychiatry residency program.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.