
Watch a brief overview of their article.
Bennett P, Brown L, Wardell L, Smelyanskaya M. Ensuring equitable vaccine distribution for COVID-19 in Wake County, North Carolina. HPHR. 2021; 30.
DOI:10.54111/0001/DD16
Public health officials in Wake County, North Carolina have been acutely aware of the disproportionate impact of COVID-19 on historically marginalized populations -Black, Hispanic, and American Indian communities. As COVID-19 vaccine rollout elsewhere in the country demonstrated that communities of color were being left behind, Wake County Human Services devised a vaccine equity strategy that aimed to increase access to and improve acceptance of COVID-19 vaccines among Black and Hispanic individuals in the county. Using epidemiological and geospatial analysis paired with community engagement activities, the strategy is currently being implemented and continuously evaluated. Its first lessons could be useful to other jurisdictions in the United States (U.S.).
Throughout the COVID- 19 pandemic, Black, Hispanic, and American Indian persons have been hospitalized at rates at least three times higher than White individuals and were at least twice as likely than their White counterparts to die of the disease (CDC, 2020a). This is unequivocally a result of systemic health inequalities rooted in the history of structural racism and exacerbated by COVID-19. Socioeconomic and psychosocial inequities such as concentrated poverty and lack of access to quality health care have made Black, Hispanic, and American Indian communities more susceptible to chronic illnesses impacting on COVID-19 morbidity (Lavizzo-Mourey & Willams, 2016; Reeves, 2020; Smith, 2018). Further, racial and ethnic wealth inequality ensured that Black, Hispanic and other individuals of color were over-represented within the ranks of front-line, essential workers and have been required to work in person, increasing exposure to COVID-19 (Pryor & Tomaskovic-Devy, 2020).
In Wake County, North Carolina Black and Hispanic communities have been disproportionally impacted by COVID-19, as seen by heightened mortality and case counts per population (NC DHHS, n.d.-a). To respond to the disparities in COVID-19 morbidity and mortality in historically marginalized populations (HMPs) – a term used to describe communities and individuals in North Carolina historically impacted by systematic exclusion, discrimination, and racism – Wake County Human Services (WCHS) used mapping, robust signup functions, and equitable distribution practices early in the COVID-19 vaccination rollout. These strategies represent only a portion of WCHS health equity plan; yet, they have the potential to impact disparities seen throughout the COVID-19 pandemic.
At the outset of 2021, healthcare providers worked diligently to meet the dual goals proposed by the Biden Administration – to administer vaccines swiftly and ensure equity (Tanne, 2021). However, initial reports of vaccine distribution showed that efficiency was outweighing equity in the majority of the states. At the beginning of March, 2021, among vaccine recipients for whom race and ethnicity data was reported 65% were White, 8.5% were Hispanic, 6.9% were Black, and 2% were American Indian or Alaska Native (CDC, 2020b). However, these numbers were not representative of the U.S. population, where 60% of individuals are White, 12.2% are Black and 18.5% are Hispanic (Kaiser Family Foundation, 2020). These challenges further reflected long-standing inequities in America’s healthcare system and underlined the need for tailored vaccination strategies for communities hardest-hit by COVID-19.
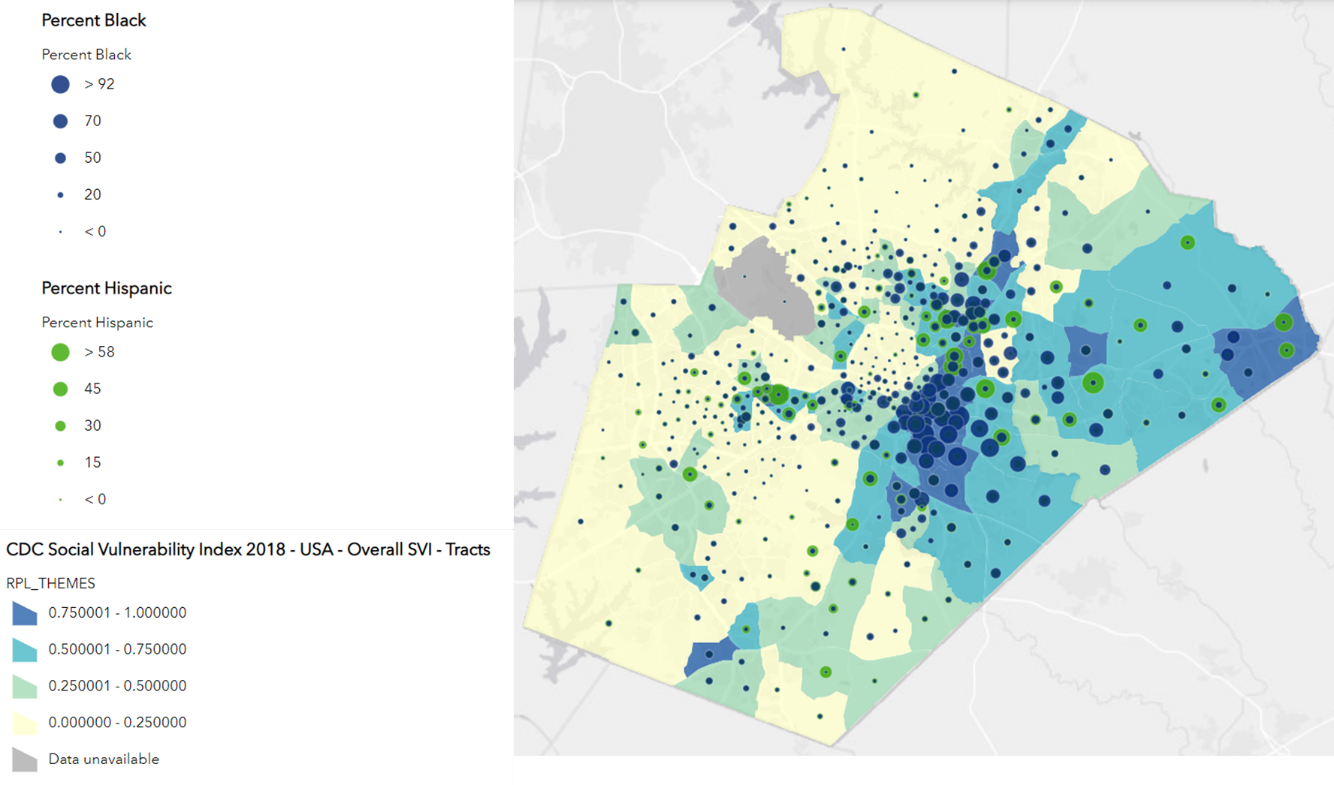
According to the recent census, Wake County is one of the fastest growing counties in the U.S and at over 1.1 million residents – one of the largest in North Carolina (Demographics, n.d.; U.S. Census Bureau, 2021). It consists of twelve municipalities, hosts the state government in the capital city of Raleigh and is home to numerous colleges and universities and three major hospital systems (Community Health Needs Assessment, n.d.). The disproportionate impact of COVID-19 on HMPs, specifically Black and Hispanic populations in Wake County is reflective of the data seen nationally. In early March, 2021, 23% of all COVID-19 cases reported in Wake County were among Hispanic individuals, though population estimates show that 10% of residents are Hispanic (U.S. Census Bureau, 2021), and 31% of all deaths attributed to COVID-19 in the county were among Black individuals (NC DHHS, n.d.-a) whereas only 21% of the county’s population identifies as Black. Additionally, the majority of COVID-19 cases were reported in areas of the county which ranked high on CDC’s social vulnerability index (SVI) scale (CDC, 2021), have higher percentage of residents who are uninsured, and host a greater percentage of Black and Hispanic individuals (Wake County GIS, 2021) (see Figure 1).
Initial data for COVID-19 vaccinations in Wake County, showed that by the first week of March out of the approximately 163,650 first doses of vaccine administered, 14.58% were received by Black individuals and 3.67% by Hispanic individuals(NC DHHS, n.d.-b). WCHS aimed to close this gap and devised a tailored approach to vaccine distribution that combined geo-targeting, prioritized registration/sign-up, and community outreach to tackle both access and hesitancy in historically marginalized communities.
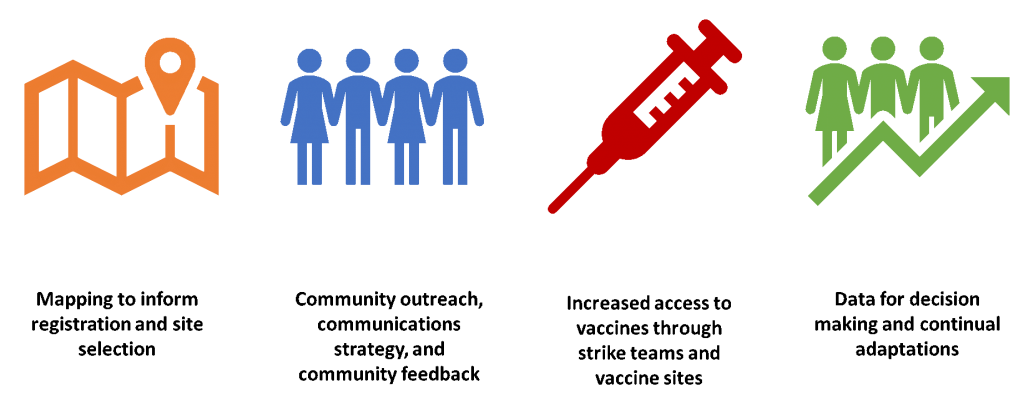
The process for ensuring vaccine equity was modeled after WCHS’s strategy for identifying and addressing testing deserts; one that was iterative and adaptive, with the aims of ensuring that the hardest hit communities were reached. Early in the pandemic, WCHS partnered with Geographic Information Systems (GIS) experts in the county’s Long Range Planning section to identify areas for semi-permanent testing site placement; this work focused on finding areas of the county where COVID-19 rates, vulnerability, and rates of under-insurance were high, yet access to testing was limited. Utilizing additional data on case positivity rates and monitoring access to testing, WCHS also rotated mobile testing sites to reach communities and individuals most impacted by COVID-19. To enhance community support for testing, the strategy also focused on complimentary outreach and messages tailored to specific audiences. While this testing intervention has not yet been documented, implementation of GIS in supporting epidemiological analysis and programmatic decision-making has been described elsewhere (Pfeiffer et al., 2008). The vaccine equity plan developed by WCHS, followed best practices learned from implementing community testing, and included components described in Figure 2.
By mid-January North Carolina activated Group Two for vaccine allocation (NC DHHS, 2021a) opening eligibility to people aged 65 and older in addition to health care workers previously activated in Group One. In advance of Group Two activation, WCHS developed a strategy to prioritize ZIP codes most impacted by COVID-19. Ten ZIP codes were identified with highest COVID-19 positivity rates, which also aligned with areas of the county with high CDC SVI, low rates of health insurance coverage and higher percentage of Black and Hispanic residents. Using ZIP codes, rather than smaller geographies (e.g. census tracts), allowed for communication of complex information to the general public. Each week, as vaccine allocations were made available to the county by North Carolina Department of Health and Human Services (NCDHHS), WCHS opened registration for eligible individuals, however appointments were not first come, first serve. Rather the county’s registration system led community members to a waitlist, with WCHS prioritizing those on the waitlist who were from the selected ten ZIP codes (see Figure 3). WCHS also ensured that registration could be accessed via the county’s webpage or via a telephone hotline to expand sign-up for those with technological barriers (Jean-Jacques & Bauchner, 2021).

Following the initial appointment allocation based on ZIP codes, further analysis was conducted to focus on census tracts within and outside the ten prioritized ZIP codes, where vulnerability, COVID-19 risk and lack of access may have been highest – this strategy was also complimented by guidance from the state of North Carolina (see below). By focusing on census tracts, WCHS was able to ensure that community outreach was tailored to specific sub-populations and that mobile strike teams – groups deployed to communities to administer vaccines – were in areas where individuals were not being reached.
As a part of its overarching community engagement strategy, WCHS has partnered with community-based organizations such as churches, non-profit partners, senior centers, Historically Black Colleges and Universities, physicians’ networks, health equity community coalitions, social justice organizations, Black Greek organizations, and youth leadership throughout the pandemic. Through this network of community partners, WCHS was able to quickly pivot to support vaccination events which expanded outreach in ZIP codes and census tracts identified through background mapping. Community outreach focused on door-to-door registration campaigns, partner-led community events, and multilingual information sessions. These outreach events utilized trusted community leaders and influencers to help provide information, connect communities to resources and increase access to vaccination opportunities. Building on lessons learned throughout the pandemic, Wake County ensured that speakers/organizations were from affected communities to garner trust, reduce hesitancy, and promote access (National League of Cities, 2021). In line with this and to further expand reach through digital platforms, WCHS hosted two COVID-19 townhalls in February – one with a panel of Black Physicians and one with trusted community leaders from the Hispanic Community in Wake County.
Allocation for vaccination doses from NCDHHS at the beginning of 2021 were provided every three weeks. Within these allocations, 60 counties with large, unvaccinated populations of HMPs and underserved communities received additional “set-aside” or “equity” doses (NC DHHS, 2021b). Given the county’s population of 1.1 million people (U.S. Census Bureau, 2021), Wake County was allocated equity doses for 25 priority census tracts. WCHS utilized these doses for community vaccine sites through strike team deployment with regional partners, as well as additional census tracts identified through background mapping. By the end February 2021, WCHS had partnered with ten community-based organizations, including religious organizations and non-profits, to host strike team events, reaching approximately 1,857 individuals for first dose vaccination events (Paige Bennett & Sutyajeet Soneja, personal communication, March 19, 2021). When possible, these sites offered wrap-around services, such as food distribution, and/or served as community testing sites to individuals who were still ineligible for vaccine, with the end goal of increased trust in community providers, as well as access and equity. Each event hosted around 200 individuals and generated substantial interest from community partners, with 16 new partners holding collaborative vaccine events through March 2021, including shelters for individuals experiencing homelessness and family violence.
In additional to strike team events, WCHS has expanded semi-permanent vaccine sites from one to three from January to March 2021. Two of the three semi-permanent sites were placed in census tracts prioritized by NCDHSS to increase access for HMPs. Criteria for site selection also included a focus on sites which are accessible by public transportation and by foot, with one of the sites housed in the WCHS Public Health building. Vaccine site location strategy was similar to WCHS’s testing strategy, which utilized community centers and local parks accessible by bus routes for residents without personal transportation. To further expand access to vaccinations, NCDHHS is providing free public transportation to vaccine sites including through GoWake Access Transportation Services — a door to door, share-ride service for qualified individuals (GoWake Access Transportation, n.d.).
As part of a longer-term plan to increase access and ensure sustainability in COVID-19 vaccinations, WCHS aims to open additional sites in each of the regions in the county.
In the national push to deliver COVID-19 vaccine to all, equity should not be compromised. Wake County officials took decisive steps to ensure HMPs in the county were prioritized early and throughout vaccine rollout. As eligibility extends, ensuring that vaccine makes it to individuals and into communities who need it most will remain WCHS priority. As the county iterates on its vaccine equity strategy, the lessons learned can inform work elsewhere.
WCHS has aimed to expand access to registration through offering platforms that do not require digital technology or Internet access. When possible, WCHS has implemented recommendations for simplifying registration practices that allowed for low-English proficiency, did not require identification or pre-registration (Jean-Jacques & Bauchner, 2021). Events hosted by community partners conducted pre-registration in advance through the partner organizations and allowed for completion of registration in the state vaccine data base on site so that community members had options outside of digital sign-up.
WCHS plans to continuously apply “data for decision making” strategies to promote vaccine equity and iterate on site selection as groups that need access or are hesitant will likely change as the county moves through mass vaccination. There is no “one size fits all” strategy to increase vaccine equity or ensure that HMPs are reached. However, WCHS plans to build on best practices used in past interventions and critically adapt to expand access to COVID-19 vaccines across the county.
Paige Bennett is the lead author of “Ensuring Equitable Vaccine Distribution for COVID-19 in Wake County, North Carolina.”
Lauren M. Brown is a global public health professional with a strong interest in promoting racial and social justice in my work, as well as working to address health inequities. Professional experience includes: 16 years leading disease surveillance and response programs in International NGO organizations, including three years leading teams during the West Africa Ebola response and five years leading community-based surveillance teams in South Sudan.
Lechelle Wilson Wardell is a Project Administrator with Wake County Human Services with nearly 30 years of experience working in Public Health. Her responsibilities include building the capacity of organizations within Wake County to address their own concerns, developing and supporting community partnerships, and providing internal consultation to programs and services of Human Services. Lechelle currently serves as the Community Outreach and Engagement Manager for COVID response, where she is responsible for addressing the disparities and disproportionalities that exist in COVID infections, hospitalizations, and deaths for historically marginalized populations.
Marina Smelyanskaya started her career in public health as an HIV testing counselor and community mobilizer in New York City. Since then, Marina’s work in the U.S. and globally remained centered around health access for communities and populations whose needs are not readily prioritized. To COVID-19 work, Marina brought almost two decades of experience in HIV and TB rooted in community engagement and inclusion.
BCPHR.org was designed by ComputerAlly.com.
Visit BCPHR‘s publisher, the Boston Congress of Public Health (BCPH).
Email [email protected] for more information.

Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of BCPHR.![]()
© 2025-2026 Boston Congress of Public Health (BCPHR): An Academic, Peer-Reviewed Journal
All Boston Congress of Public Health (BCPH) branding and content, including logos, program and award names, and materials, are the property of BCPH and trademarked as such. BCPHR articles are published under Open Access license CC BY. All BCPHR branding falls under BCPH.
Use of BCPH content requires explicit, written permission.